To craft a new color-switching material, scientists have again taken inspiration from one of nature’s masters of disguise: the chameleon.
Thin films made of heart cells and hydrogel change hues when the films shrink or stretch, much like chameleon skin. This material, described online March 28 in Science Robotics, could be used to test new medications or possibly to build camouflaging robots.
The material is made of a paper-thin hydrogel sheet engraved with nanocrystal patterns, topped with a layer of living heart muscle cells from rats. These cells contract and expand — just as they would inside an actual rat heart to make it beat — causing the underlying hydrogel to shrink and stretch too. That movement changes the way light bounces off the etched crystal, making the material reflect more blue light when it contracts and more red light when it’s relaxed. This design is modeled after nanocrystals embedded in chameleon skin, which also reflect different colors of light when stretched (SN Online: 3/13/15).
When researchers treated the material with a drug normally used to boost heart rate, the films changed color more quickly — indicating the heart cells were pulsating more rapidly. That finding suggests the material could help drug developers monitor how heart cells react to new medications, says study coauthor Luoran Shang, a physicist at Southeast University in Nanjing, China. Or these kinds of films could also be used to make color-changing skins for soft robots, Shang says.
The center of the Milky Way may be abuzz with black holes. For the first time, a dozen small black holes have been spotted within the inner region of the galaxy in an area spanning just a few light-years — and there could be thousands more.
Astrophysicist Charles Hailey of Columbia University and his colleagues spotted the black holes thanks to the holes’ interactions with stars slowly spiraling inward, the team reports in Nature on April 4. Isolated black holes emit no light, but black holes stealing material from orbiting stars will heat that material until it emits X-rays. In 12 years of telescope data from NASA’s orbiting Chandra X-ray Observatory, Hailey and colleagues found 12 objects emitting the right X-ray energy to be black holes with stellar companions. Based on theoretical predictions of how many black holes are paired with stars, there should be up to 20,000 invisible solo black holes just in that small part of the galaxy. The discovery follows decades of astronomers searching for small black holes in the galactic center, where a supermassive black hole lives (SN: 3/4/17, p. 8). Theory predicted that the galaxy should contain millions or even 100 million black holes overall, with a glut of black holes piled up near the center (SN: 9/16/17, p. 7). But none had been found. “It was always kind of a mystery,” Hailey says. “If there’s so many that are supposed to be jammed into the central parsec [about 3.26 light-years], why haven’t we seen any evidence?” Finding the 12 was “really hard,” he admits.
It’s unclear how the black holes got to the galaxy’s center. Gravity could have tugged them toward the supermassive black hole. Or a new theory from Columbia astronomer Aleksey Generozov suggests black holes could be born in a disk around the supermassive black hole.
The researchers ruled out other objects emitting X-rays, such as neutron stars and white dwarfs, but acknowledged that up to half of the sources they found could be fast-spinning stellar corpses called millisecond pulsars rather than black holes. That could add to the debate over whether a mysterious excess in gamma rays at the galactic center is from pulsars or dark matter (SN: 12/23/17, p. 12).
“The theorists are going to have to slug it out and figure out what’s going on,” Hailey says.
Every few years, a buzz fills the air in the southeastern United States as adolescent cicadas crawl out from the soil to molt and make babies. After a childhood spent sipping tree sap underground, some species emerge every 13 years, others every 17 years, rarely overlapping. Yet somehow in this giant cicada orgy, hybridization happens between species that should be out of sync.
Researchers have sought to explain how the two life cycle lengths developed. A new study published online April 19 in Communications Biology fails to pin the difference on genetics, but finds some interesting things along the way. Cicadas fall into three species groups that diverged from one another about 3.9 million to 2.5 million years ago. Within each of those groups, species on a 13-year schedule diverged from 17-year-cycle cicadas about 200,000 to 100,000 years ago, the researchers from the United States and Japan report.
But the researchers also found that the 17-year and 13-year broods within each group share genetic code — evidence of hybridization. It’s possible that neighboring broods swapped DNA when their emergence overlapped — something that happens every 221 years — or if stragglers emerged early or late.
Everybody agrees that medical treatments should be based on sound evidence. Hardly anybody agrees on what sort of evidence counts as sound.
Sure, some people say the “gold standard” of medical evidence is the randomized controlled clinical trial. But such trials have their flaws, and translating their findings into sound real-world advice isn’t so straightforward. Besides, the best evidence rarely resides within any single study. Sound decisions come from considering the evidentiary database as a whole. That’s why meta-analyses are also a popular candidate for best evidence. And in principle, meta-analyses make sense. By aggregating many studies and subjecting them to sophisticated statistical analysis, a meta-analysis can identify beneficial effects (or potential dangers) that escape detection in small studies. But those statistical techniques are justified only if all the studies done on the subject can be obtained and if they all use essential similar methods on sufficiently similar populations. Those criteria are seldom met. So it is usually not wise to accept a meta-analysis as the final word.
Still, meta-analysis is often a part of what some people consider to be the best way of evaluating medical evidence: the systematic review.
A systematic review entails using “a predetermined structured method to search, screen, select, appraise and summarize study findings to answer a narrowly focused research question,” physician and health care researcher Trisha Greenhalgh of the University of Oxford and colleagues write in a new paper. “Using an exhaustive search methodology, the reviewer extracts all possibly relevant primary studies, and then limits the dataset using explicit inclusion and exclusion criteria.”
Systematic reviews are highly focused; while hundreds or thousands of studies are initially identified, most are culled out so only a few are reviewed thoroughly with respect to the evidence they provide on a specific medical issue. The resulting published paper reaches a supposedly objective conclusion often from a quantitative analysis of the data. Sounds good, right? And in fact, systematic reviews have gained a reputation as a superior form of medical evidence. In many quarters of medical practice and publishing, systematic reviews are considered the soundest evidence you can get.
But “systematic” is not synonymous with “high quality,” as Greenhalgh, Sally Thorne (University of British Columbia, Vancouver) and Kirsti Malterud (Uni Research Health, Bergen, Norway) point out in their paper, accepted for publication in the European Journal of Clinical Investigation. Sometimes systematic reviews are valuable, they acknowledge. “But sometimes, the term ‘systematic review’ allows a data aggregation to claim a more privileged position within the knowledge hierarchy than it actually deserves.”
Greenhalgh and colleagues question, for instance, why systematic reviews should be regarded as superior to “narrative” reviews. In a narrative review, an expert in the field surveys relevant publications and then interprets and critiques them. Such a review’s goal is to produce “an authoritative argument, based on informed wisdom,” Greenhalgh and colleagues write. Rather than just producing a paper that announces a specific conclusion, a narrative review reflects the choices and judgments by an expert about what research is worth considering and how to best interpret the body of evidence and apply it to a variety of medical issues and questions. Systematic reviews are like products recommended to you by Amazon’s computers; narrative reviews are birthday presents from friends who’ve known you long and well.
For some reason, though, an expert reviewer’s “informed wisdom” is considered an inferior source of reliable advice for medical practitioners, Greenhalgh and colleagues write. “Reviews crafted through the experience and judgment of experts are often viewed as untrustworthy (‘eminence-based’ is a pejorative term).”
Yet if you really want the best evidence, it might be a good idea to seek the counsel of people who know good evidence when they see it.
A systematic review might be fine for answering “a very specific question about how to treat a particular disease in a particular target group,” Greenhalgh and colleagues write. “But the doctor in the clinic, the nurse on the ward or the social worker in the community will encounter patients with a wide diversity of health states, cultural backgrounds, illnesses, sufferings and resources.” Real-life patients often have little in common with participants in research studies. A meaningful synthesis of evidence relevant to real life requires a reviewer to use “creativity and judgment” in assessing “a broad range of knowledge sources and strategies.”
Narrative reviews come in many versions. Some are systematic in their own way. But a key difference is that the standard systematic review focuses on process (search strategies, exclusion criteria, mathematical method) while narrative reviews emphasize thinking and interpretation. Ranking systematic reviews superior to narrative reviews “elevates the mechanistic processes of exhaustive search, wide exclusion and mathematical averaging over the thoughtful, in-depth, critically reflective processes of engagement with ideas,” Greenhalgh and collaborators assert.
Tabulating data and calculating confidence intervals are important skills, they agree. But the rigidity of the systematic review approach has its downsides. It omits the outliers, the diversity and variations in people and their diseases, diminishing the depth and nuance of medical knowledge. In some cases, a systematic review may be the right approach to a specific question. But “the absence of thoughtful, interpretive critical reflection can render such products hollow, misleading and potentially harmful,” Greenhalgh and colleagues contend.
And even when systematic reviews are useful for answering a particular question, they don’t serve many other important purposes — such as identifying new questions also in need of answers. A narrative review can provide not only guidance for current treatment but also advice on what research is needed to improve treatment in the future. Without the perspective provided by more wide-ranging narrative reviews, research funding may flow “into questions that are of limited importance, and which have often already been answered.”
Their point extends beyond the realm of medical evidence. There is value in knowledge, wisdom and especially judgment that is lost when process trumps substance. In many realms of science (and life in general), wisdom is often subordinated to following rules. Some rules, or course, are worthwhile guides to life (see Gibbs’ list, for example). But as the writing expert Robert Gunning once articulated nicely, rules are substitutes for thought.
In situations where thought is unnecessary, or needlessly time-consuming, obeying the rules is a useful strategy. But many other circumstances call for actual informed thinking and sound judgment. All too often in such cases the non-thinkers of the world rely instead on algorithms, usually designed to implement business models, with no respect for the judgments of informed and wise human experts.
In other words, bots are dolts. They are like a disease. Finding the right treatment will require gathering sound evidence. You probably won’t get it from a systematic review.
Genetic modifications to a plant that makes artemisinin, a key compound used in malaria drugs, more than tripled the amount of the ingredient naturally produced in leaves.
Previous attempts to genetically engineer Artemisia annua to increase the yield of artemisinin had failed. So Kexuan Tang, a plant scientist at Shanghai Jiao Tong University, and colleagues determined A. annua’s entire genetic instruction book and identified three genes crucial to artemisinin production. Genetic modifications to increase the activity of these genes boosted the artemisinin level in leaves from 0.1–1 percent of their dry weight to 3.2 percent, the researchers report April 24 in Molecular Plant. Malaria kills about 440,000 people worldwide every year. The scientists hope to save lives by increasing and stabilizing the global supply of artemisinin, which has been in shortage due to unstable supply, Tang says. Seeds of these modified plants have been shipped to Madagascar, which grows the most A. annua in Africa, as part of a field trial.
“This is a milestone paper for artemisinin,” says Akhil Vaidya, an immunologist at Drexel University in Philadelphia who was not involved in the research. Artemisinin was discovered by Chinese chemist Youyou Tu in 1972, as she was investigating thousands of traditional Chinese remedies. The discovery, which has saved millions of lives, earned her the 2015 Nobel Prize in medicine (SN Online: 10/5/15).
Drug companies have used genetically modified yeast to produce semisynthetic artemisinin (SN: 5/4/13, p. 20), which is also effective against malaria. But artemisinin from plants is cheaper, Vaidya says. “Let the sun shine. Let the plants do their job,” he says.
Toastier nest temperatures, rather than sex chromosomes, turn baby turtles female. Now, a genetic explanation for how temperature determines turtles’ sex is emerging: Scientists have identified a temperature-responsive gene that sets turtle embryos on a path to being either male or female. When researchers dialed down that gene early in development, turtle embryos incubating at the cooler climes that would normally yield males turned out female instead, researchers report in the May 11 Science.
Scientists have struggled since the 1960s to explain how a temperature cue can flip the sex switch for turtles and other reptiles (SN Online: 1/8/18). That’s partly because gene-manipulating techniques that are well-established in mice don’t work in reptiles, says study coauthor Blanche Capel, a developmental biologist at Duke University School of Medicine. Previous studies showed certain genes, including one called Kdm6b, behaving differently in developing male and female turtles. But until recently, nobody had been able to tweak those genes to directly test which ones controlled sex. “This is the first venture down that path,” says Clare Holleley, an evolutionary geneticist at the Australian National Wildlife Collection in Canberra who wasn’t part of the study. “It’s really quite a breakthrough.”
In the new study, Capel’s lab collaborated with a group of Chinese researchers led by Chutian Ge of Zhejiang Wanli University in Ningbo. Ge’s team recently developed a way to lessen the activity of particular reptilian genes by injecting viruses bearing snippets of artificial RNA into developing eggs.
The researchers used the technique to weaken the effects of the Kdm6b gene in the embryos of red-eared slider turtles (Trachemys scripta elegans) before the gonads formed, then tracked the embryos’ development at 26° Celsius.
“To my delight, it resulted in complete sex reversal,” Capel says. That temperature should have yielded all male turtles. Instead, in two separate experiments done with different gene-silencing viruses, 80 and 87 percent of the surviving embryos became female. Still, something as complex as sex determination can’t be boiled down to a single gene. Kdm6b controls a gene called Dmrt1, which had already been shown to direct male development, Capel’s team also found. And while Kdm6b does behave differently as temperatures rise, it doesn’t show the same response in all tissues. That suggests that the gene doesn’t directly sense temperature, but is instead receiving messages from some higher-up gene that reacts directly to temperature and directs Kdm6b’s behavior in different tissues, the researchers propose.
Whether Kdm6b plays the same role in other reptiles remains to be seen. A 2017 study in Science Advances coauthored by Holleley found that the gene influenced bearded dragons’ sexual fate (SN Online: 6/14/17). But other genes in the same family, Jumonji genes, are also known to influence development in both reptiles and mammals. And those genes might not work exactly the same way in other reptiles.
“There’s this huge diversity of sex determining modes in reptiles,” Holleley says. Even if Kdm6b is an important switch in other reptiles, “the genes that Jumonji genes are activating are probably going to be different in every reptile.”
There are other wrinkles, too. “This is really exciting finding, but we need to remember that everything in a lab is controlled,” says Itzel Sifuentes-Romero of Florida Atlantic University in Boca Raton. Wild turtle eggs are subject to fluctuations in temperature and moisture as they incubate, she says, which means the signals that temperature-sensitive genes are receiving are far more muddled.
A new analysis of satellite images and seismic waves from North Korea’s nuclear test site support theories that the underground facility has at least partially collapsed.
Seismologists across the world have been tracking the clandestine nuclear weapons program for years by analyzing vibrations that emanate from explosions at the test site under Mount Mantap (SN: 8/5/17, p. 18). Now, researchers have paired 3-D satellite images of Mount Mantap with seismic tremor data to simulate how the mountain’s interior might have changed after a hydrogen bomb test on September 3, 2017. The simulations indicate that the blast — which triggered an earthquake of estimated magnitude 6.3 — caused a cave-in directly above the detonation site, researchers report online May 10 in Science. The simulations also suggest that a second rock collapse, about 700 meters south of the detonation site, caused a smaller quake about eight minutes after the initial explosion.
These rock falls, which caused the face of Mount Mantap to sink about 0.5 meters, could have buried part or all of the underground test facility, rendering it unusable, says study coauthor Teng Wang, a remote sensing and geodesy researcher at the Earth Observatory of Singapore.
The results support another seismic analysis published online April 27 in Geophysical Research Letters suggesting an underground collapse at Mantap. That study led some media to speculate that North Korea didn’t pledge in April to halt nuclear testing because of international pressure, but because the test site could no longer be used.
Ultimately, experts would have to inspect the site to confirm that the Mount Mantap facility is out of order, says study coauthor Douglas Dreger, an earth and planetary scientist at the University of California, Berkeley. “It’s really hard to make that judgment call without having information at that site — getting boots on the ground and investigating it.”
In Nevada, 40,000 people are stepping up to the cutting edge of precision medicine. They are getting their DNA deciphered by the testing company Helix. The idea of the Healthy Nevada project is to link genetic and medical data with information about the environment to get a clearer picture of all the factors that influence health. The free tests are going like hot cakes.
When the Healthy Nevada project launched a similar partnership with 23andMe in 2016, 5,000 residents were offered a free testing kit in exchange for participation in the program.
“Within 24 hours, 5,000 people had broken our website and signed up really enthusiastically,” says project head Joseph Grzymski, a computational biologist at the Desert Research Institute’s Reno campus. Another 5,000 kits were offered up. “Within 24 hours that sold out,” Grzymski says, “and we had 4,000 people on a waiting list.”
Even without an invitation or a free deal, consumers are flocking to these tests. Last year, more than 7 million people, mostly in the United States, sent their DNA to testing companies, according to industry estimates. DNA testing is no longer a niche interest, it’s a mass consumer market, with millions of people wanting to experience the emotionally powerful, life-affirming discoveries that can come from simply spitting in a tube,” Howard Hochhauser, interim chief executive of the online geneaology testing company Ancestry, said in a public statement about the company’s 2017 holiday sales.
I am one of those 7 million who wanted a read on my DNA, to learn about myself and my heritage. And I went all out. My DNA is now part of the data banks of consumer genetic testing companies Ancestry, 23andMe, Family Tree DNA, Gencove, Genos, Helix, Living DNA and Veritas Genetics. (For a review of my experiences, click here). I learned some things about myself — and about the glaring limits of today’s consumer genetic tests. Broad business Companies claim that they can read nearly everything about a person in his or her DNA profile. Some firms use DNA details to trace family trees or offer dietary advice and training regimens for burning fat or building muscle. Others go further out on a limb, claiming that testing a handful of genes can reveal a child’s future potential. Need help choosing a wine? A test of variants in a few genes associated with taste and smell — along with a quick quiz — offers options that one company says will please your palate. There are even kits that claim to reveal superhero abilities, or that let two friends virtually mash up their DNA to see what their offspring might look like.
While some applications are clearly frivolous or pure entertainment, others are serious medical business. Consumers can buy tests that screen for gene variants that increase risk for developing cancer, high cholesterol, diabetes, Alzheimer’s disease or Parkinson’s. Human Longevity, in San Diego, pairs a readout of a person’s whole genome with extensive body imaging, blood tests and other medical screening to gauge a client’s health with the goal of increasing life span. Scientists say it’s probably going to take this sort of comprehensive information to really personalize medicine, but few people can afford Human Longevity’s $25,000 price tag. These companies are part of a growing trend often called personalized, or precision, medicine. Health care systems, including national systems in Estonia, Finland, England and elsewhere, are adding DNA data to medical records, hoping to better tailor treatments to individual patients or even prevent illness. Consumer testing companies draw on databases compiled from such publicly funded research resources to make predictions about a customer’s health.
Some testing companies share their data with researchers who study human health and genetics, some do their own studies and some use the data as a revenue source, selling it to pharmaceutical companies. I opted to allow the companies to share my data with researchers. You don’t have to choose that option, but I like the idea of contributing to science.
And more research is needed. Scientists still haven’t really learned how to interpret the story in a person’s genetic instruction book, or genome, and apply it to an individual’s health care. Every researcher I talked to says that goal is far in the future. “There will be a time when many more common health conditions will have tests you can do that will really inform you,” says Bryce Mendelsohn, a medical geneticist at the University of California, San Francisco. “But it will be years, years, decades before we’re really at that stage.”
In August, Mendelsohn opened the Preventive Genomics Clinic at UCSF’s Benioff Children’s Hospital. There, he counsels adults on what type of genetic testing is right for them, and what to expect from the results. He’s not against consumer genetic testing, but he tells his patients that it’s for entertainment purposes only.
“If they say, ‘I want to know about my ancestry. I want to know how much Neandertal I have,’ I say, ‘Great, that’s what consumer genetic testing is for.’ ”
But for medically relevant information — such as genetic variants that increase risk for cancer, high cholesterol or heart problems — Mendelsohn orders tests from labs that are certified to make thorough clinical diagnoses. And he makes sure his patients know what to expect and what their results mean.
“It’s not that companies that are selling tests are somehow evil,” Mendelsohn says; they just promise too much. “I just tell people up front, if you’re going to get this test, the odds are that you’re going to come back with nothing.”
False security Daniel Cressman, a commercial real estate broker in San Francisco, wasn’t expecting to get any troubling or surprising results when he decided to have his DNA deciphered. He did it “just out of curiosity” after attending a conference on future trends. He wanted to be on the leading edge of what he sees as the wave of the future. One day soon, he predicts, “You’ll go to the doctor and the first thing they’ll do is pull up your genome.”
After hearing about the different levels of genetic testing that are offered (see “How much gets tested?”), Cressman decided he wanted the thorough approach: whole genome sequencing. To have his full genetic instruction book deciphered, rather than only certain parts, he looked into various companies’ offerings and ultimately settled on Veritas Genetics. The company will sequence a person’s genome for $999. Other companies offer whole genome sequencing, too, but for a higher price tag, anywhere from $1,295 for genealogy purposes to health testing ranging from $2,500 to more than $25,000.
Some of Cressman’s family and friends are not on board with genetic testing, he says. “Some people ask, ‘What if you discover something you don’t want to know?’ ” But Cressman thinks it’s usually better to know what’s potentially in store. “If I’m flying San Francisco to New York on an Airbus and there’s a crack in the wing, I’d kind of like to know before I get on the plane.” He didn’t discover any cracks in his genes that would cause him or his doctor concern. “Nothing popped out at all,” he says.
Like Cressman’s, my DNA’s story, based on Veritas’ whole genome sequencing, turned out to be pretty boring. For both of us, testing didn’t turn up any variations embedded in our DNA that are likely to cause us to develop a genetic disease. That’s good news, says clinical medical geneticist Gail Jarvik. “We tell people, ‘If you’re lucky, you have a boring genome. That’s what you really want.’ ”
But just because Veritas didn’t find anything scary in our genomes, doesn’t mean Cressman and I won’t develop health problems. Getting a clean bill of health based on your genes “can be very misleading and falsely reassuring,” says Jarvik, who heads the division of medical genetics at the University of Washington in Seattle. It can also be a bit of a letdown for people who expect revelations.
I admit to wanting more. Maybe I should have known better, but I thought I’d find out about all the ways I differ from other people, those genetic quirks that make me, me. I was most excited to learn about one weird thing: why my face flushes flaming red and I itch all over when I have even a few sips of alcohol. The companies advertised that they could reveal the genetic reason behind the annoying reaction. When the results came back, I was baffled. 23andMe and Veritas both said that I am unlikely to flush when I take a drink.
But those companies based their erroneous assertion on a variant known to be associated with alcohol-flushing in East Asians. My background is European, so it’s unlikely that I would have that variant in the first place. I might have a different variant in that same gene or in some other gene related to how my body processes alcohol. Neither company reports on the other genes. So maybe I was expecting too much. But maybe that’s not entirely my fault.
“I think [consumers are] being overpromised that getting the genome sequenced will tell them lots of things that it won’t,” Jarvik says. “I’ve definitely run across people who have … been very disappointed because they didn’t learn as much as they thought.” No drama Most healthy people who send off their cheek swabs or saliva samples for DNA testing should expect to have a boring genome, says Leslie Biesecker, a molecular and clinical geneticist at the National Institutes of Health in Bethesda, Md. At this stage of the science, genome sequencing is not very useful for most people, he says.
DNA sequencing does play a role in diagnosing mysterious inherited diseases and for detecting the mutations that lead to cancer, Biesecker says. But he’s dubious of the value for healthy people. “If you don’t have such a condition, there’s a much lower chance of finding something that would be useful to you medically.”
Only a very few people may have a rare genetic disorder and not know it, Biesecker says. “Occasionally we pick up some really severe stuff — hearing loss, cancer susceptibility or severe heart conditions — that you do need to do something about,” he says. “We’ve had several people with a pretty high susceptibility to colon cancer, and we know it will add 10 to 20 years to their life expectancy if they get annual colonoscopies. So for those people, it’s clear, it’s dramatic and it’s useful.” But such powerful results are the exception.
Roughly 3 percent of healthy people have known disease-causing variants in one or more of 59 genes on a list compiled by the American College of Medical Genetics and Genomics, according to a 2015 report in Genetics in Medicine. Variants in those genes are considered “medically actionable.” In other words, the genetic variants could cause problems for which medications, screening or other steps can be taken to ease or head off symptoms and serious consequences.
To get results on most of those medically important variants, according to U.S. Food and Drug Administration rules, a person needs a doctor to sign off, which is why Veritas requires a doctor’s order before it will analyze a DNA sample.
Last year, the FDA opened the door a crack for one direct-to-consumer company, 23andMe, to offer customers information about diseases related to particular changes in individual genes — no prescription or referral needed. For example, the company can now tell customers whether they have one of three variants in the BRCA1 and BRCA2 genes that raise the risk of breast cancer. (There are thousands of variants in those genes linked to breast cancer, but the company is allowed to report on only three.)
Customers who want to know can also find out if they have a variant of the APOE gene linked to a higher chance of getting Alzheimer’s disease, or variants in the LRRK2 and GBA genes associated with Parkinson’s disease. The company can also tell you about genetic variants that increase the risk of the eye disease macular degeneration, as well as celiac disease and some other health conditions with well-established genetic connections. All without a referral or prescription. Carried away People inherit two copies of most genes — one from mom, one from dad. Many of the variants on the list of 59 genes cause trouble when just a single copy is inherited from one parent. Geneticists refer to such genetic variants as “dominant.”
Some dominant variants lead to rare conditions, including changes in the BRCA1 and BRCA2 genes that can cause breast and ovarian cancers, a variant of the PCSK9 gene that causes high cholesterol and changes in multiple genes that increase colon cancer risk. Some genetic variants linked to certain heart problems, neurological disorders and other serious health issues are also on the list.
Most people, including me, probably don’t have defects in single genes that could bring on a health crisis. What we pass on to our children, though, is another matter. Many people carry one copy of a disease-causing mutation, which isn’t enough to cause trouble for them, but they could pass it on to their children. A child who inherits disease-causing versions of the same gene from both parents could be very sick. That’s the case for conditions such as cystic fibrosis, phenylketonuria, Tay-Sachs and many other “recessive” genetic diseases.
23andMe, Veritas and other direct-to-consumer genetic testing companies can now give information about a person’s “carrier status,” identifying whether you have one copy of a recessive disease variant that your kids could inherit.
Preliminary studies suggest that, on average, most people are carriers for two recessive genetic diseases — some carry no such variants, others have up to seven or eight. I’m average. I carry two, or three, depending on the company doing the test; I didn’t get the same results from every company.
Being a carrier for a life-threatening genetic disease could influence a person’s decisions about having children. When both members of a couple carry disease-causing variants in the same gene, the couple has a 25 percent chance of having an affected child. Some couples might risk it; others might forgo having children. Some may try to improve their odds of having a healthy baby by seeking help from fertility clinics, where doctors can perform in vitro fertilization and then screen out embryos that have inherited two copies of the disease-causing variant (SN: 12/23/17, p. 21). Reality check Unlike the rare single-gene diseases, the vast majority of common traits, diseases and conditions are the product of tweaks in many genes working together. Such conditions are called polygenic traits. Researchers aren’t yet very good at figuring out how all the subtle tweaks in the genome, called single nucleotide polymorphisms, or SNPs, come together to affect appearance, behavior and health.
Take type 2 diabetes, for instance. Hundreds of gene variants have been linked to the disease, but none is the single factor that ensures a person will develop the disorder. Most SNPs have only a tiny influence on the chance a person will get a disease — lifestyle and environment play a role, too.
And what should a person do about a variant that nudges up diabetes risk? Biesecker told me how it might play out. “If I do have that variant, I can go to my doctor [who] will tell me I can improve my health by improving my diet and exercising,” he says. “If I don’t have that variant, I can go to my doctor and my doctor will say, ‘You can improve your health and longevity by improving your diet and exercising.’ ” If you get the same advice either way, there’s little value in knowing whether you have the variant or not, he says.
Companies such as 23andMe used to tell consumers their risk of developing polygenic diseases. No more. In 2013, the FDA banned the company from giving customers in the United States that information. Right now, Veritas, which is certified to give clinical information, doesn’t report risk of diseases that are influenced by multiple genes. It and other companies are allowed to tell customers about polygenic traits that aren’t disease-related, such as hair and eye color or attached or detached earlobes. 23andMe examines 32 variants to weigh in on whether your earlobes hang free or cling to the side of your head. And as many as 49 different spots in the genome could be involved in earlobe shape, a study published last year in the American Journal of Human Genetics suggests. That study included data collected from 23andMe customers. This kind of information lands on the fun-but-frivolous end of the information spectrum. But it’s kind of cool to learn the genetics behind your ear shape.
Plenty of companies claim they can read your genes to tell you what you should eat or how you should exercise. Basing your diet on science seems like the smart thing to do. But Christopher Gardner, director of nutrition studies at Stanford University’s Prevention Research Center, says no. “Not today.”
Gardner should know. He and colleagues tested whether variants in three genes involved in fat or carbohydrate metabolism could predict whether a person would be more successful at losing weight on a low-fat or a low-carb diet. The idea was based on his team’s previous study of 130 people. Those whose genetic profile matched the diet they were assigned to lost three times as much weight as those whose diets and genetics didn’t match. “It was plausible,” Gardner says. So the team expanded the study to more than 600 overweight and obese people, assigning each person at random to either a low-fat or low-carb diet. After one year, the researchers looked at weight loss among participants: Did a diet based on an individual’s genetics make a difference?
“The punch line is really short,” Gardner says. “It didn’t work.” On average, participants in both diet groups lost about five or six kilograms (12 to 13 pounds) over 12 months. Some lost much more, some less and some gained weight. But there was no connection between successful weight loss and whether the participants’ diet and gene profiles matched, Gardner and colleagues reported in the Feb. 20 JAMA.
I pointed out that consumer genetic companies usually include the variants Gardner and colleagues tested, plus four or five other variants related to body mass index, having a sweet tooth and sensitivity to insulin, the hormone that regulates blood sugar. Would that be better?
“No,” Gardner says. “You can make a plausible claim, but then you have to test it.”
Obesity is a complex trait. Studies have linked more than 200 variants to body weight, but none tell the whole story of why people’s weight varies so much. “It isn’t that there’s one answer and in 10 years [we’ll have it],” Gardner says. “The answers will get progressively clearer and clearer. We could have a couple next year. They just won’t be the end-all, be-all answers.”
Drug reactions If genetic testing can’t tell you much about health, diet and exercise, what is it good for? Even the most skeptical researchers I talked with said that one area holds promise: pharmacogenetics, or how variants in DNA affect how people will react to certain drugs. David Bick, a clinical geneticist at the HudsonAlpha Institute for Biotechnology in Huntsville, Ala., has sequenced 45 people’s genomes as part of a new program. The mostly white, highly educated, middle-aged participants, ranging in age from 31 to 89, paid about $7,000 for thorough physical exams along with DNA sequencing and analysis. HudsonAlpha collaborates with Huntsville-based Kailos Genetics to give participants pharmacogenetic rundowns. These drug reaction profiles will be invaluable for future reference, Bick says.
For example, doctors often prescribe a drug called clopidogrel, brand name Plavix, to people who have survived a heart attack. The drug keeps blood clots from forming, reducing the risk of another heart attack. In the body, the drug has to be converted to an active form by several enzymes, including CYP2C19. “If you have a change in that CYP2C19 gene, you can’t convert [Plavix] to the active form,” Bick says. If you have a heart attack and your doctor knows you have the variant, you could get a different medication that works for you, he explains.
We all have about an 80 percent chance of having at least one genetic variant in one of 806 genes that could alter the way one of the top 100 prescribed drugs in the United States works, researchers reported December 22 in Genome Medicine.
Based on my Veritas report, the only one that gave this information, I have at least 48 variants that can influence my reaction to dozens of drugs, all but one of which I don’t take. So the information isn’t that useful right now, but it may be useful in the future.
Maybe it isn’t so helpful today, but don’t dismiss genetic testing out of hand, says Robert Green, a geneticist who has been studying people’s responses to genetic information for more than two decades. Green, of Brigham and Women’s Hospital in Boston, thinks scientists will soon have a better handle on genetic information. “What we see today is not the endgame. It’s not even the second inning.”
Direct-to-consumer genetic testing first came on the market about a decade ago, but I resisted the temptation to see what health information is hidden in my DNA — until now.
As a molecular biology writer, I’ve been skeptical that the field of genetics is mature enough to accurately predict health (see related article). What finally motivated me to send away my DNA in the mail was the fact that companies are now offering much more genetic information. Is more better? Would an expensive test that deciphered my entire genetic instruction manual, or genome, reveal more about me than more limited tests? That’s what I wanted to find out.
For health testing, I sent spit samples to 23andMe, Genos and Veritas Genetics, three companies that represent the various levels of DNA testing available to consumers. (I did ancestry testing, too; you can read about my experiences with that in June.) These companies all analyze natural spelling variations in the string of letters that make up DNA. Where most people have, say, a “G,” some might have an “A.” Most of these genetic variants are harmless, but some raise the risk for certain diseases.
Where these companies differ is in how much of the genome they assess and whether they look for only a limited set of known variants or can uncover new ones specific to an individual. Getting started The DNA-testing process starts off the same for all of the companies I tried: ordering a kit online. Genos and Veritas both require a doctor to sign off on the test. 23andMe doesn’t, and as a result, the U.S. Food and Drug Administration limits the medical information the company can report. My doctor reluctantly agreed, but only because I was exploring DNA testing as part of my job. She said there was nothing in my personal health records or family history that would normally lead her to order a genetic test.
The kits all contained the same type of saliva-collection tubes. Sample prep was easy — register the kit’s number online, spit in a tube, mail in the sample. I also opted to let each company use my DNA in research studies, which required an extra step of answering a questionnaire about myself.
Within a couple of months, 23andMe and Genos emailed to tell me my results were available online. Because of a technical glitch, it took about seven months to get results from Veritas. The company says the typical wait time is closer to 12 weeks. Veritas also sent a copy of its report to my doctor.
23andMe 23andMe uses the oldest technology, called SNP genotype testing. SNPs, short for single nucleotide polymorphisms, are the spelling variations in DNA. For $199, 23andMe examines about 690,000 predetermined SNPs. That may sound like a lot, but it’s only 0.01 percent of the 6 billion DNA letters in the human genome. It’s the genetic equivalent of spot-checking a few letters in each chapter of War and Peace and trying to decipher the plot. Still, the company can tell you interesting things about some physical and physiological traits, like cleft chins, dimples or the ability to taste bitter flavors. And 23andMe has FDA approval to report on a few health conditions linked to specific genetic variants, such as celiac disease and macular degeneration.
The problem is, the company tests only a small subset of all potential SNPs. Getting a report of “variants not detected” doesn’t mean you don’t have any variants related to a particular medical condition. It just means you don’t have the ones tested for.
On the plus side, 23andMe provides clear explanations of what it does and doesn’t test for, and lists other factors that contribute to disease risk. In fact, 23andMe does a far better job than Genos or Veritas of explaining what having specific genetic variants means.
Genos Genos offers broader testing, for $499. It reads, or “sequences,” every letter in a person’s protein-producing genes. By deciphering this Cliffs Notes version of the genome, called the exome, Genos can theoretically find genetic changes that are unique to an individual, though the significance of these finds for health isn’t always clear. Compared with the other two services, Genos gave me the most data but the least useful information. The company found 44,225 variants in my exome and showed me how many are on each chromosome. But Genos provided information for just 4,294 of them because those variants are in ClinVar, the publicly available database that Genos draws information from.
And even for these variants, Genos gave few details — like how common the variants are and whether they change one of my proteins. The company offered almost no interpretation of what the variants mean for my health, other than to classify how harmful they might be: pathogenic, likely pathogenic, likely benign, benign or unknown significance. Most frustrating, Genos didn’t tell me which diseases these variants are associated with. I would need to explore the scientific literature myself to figure this out. So for most people, Genos’ report wouldn’t be that useful.
The company did, however, have more to say about how my variants influence a variety of my traits, such as hair and eye color, freckling, several characteristics of my ears and my ability to smell cut grass, roses and sweat. Genos also reports how genetics can affect a few behavioral characteristics, such as a tendency to overeat and the propensity to worry.
Veritas Genetics Finally, Veritas charged $999 to read nearly every letter in my genome, including portions in between genes that regulate gene activity and parts containing noncoding RNAs, which do a variety of cellular jobs. Those sections between genes are proving to be lush territory for discovering health risks. Not surprisingly, Veritas gave me the most wide-ranging report. For instance, only Veritas shared “pharmacogenomic” information — how my genetic variants could influence how certain drugs affect me. The list of drugs my genes may or may not play well with is long. I take only one drug on the list, but I’m glad to have all of this information in case it becomes relevant in the future.
While Veritas has nearly the entirety of my genetic information in its data banks, the company told me surprisingly little. Turns out, I’m just not that interesting, genetically speaking. The company screened more than 40,000 genes (including the noncoding RNAs) but found no big health risks — at least, none that scientists can reliably predict today.
The company did cover a more extensive list of physical and physiological traits than either Genos or 23andMe did. Veritas’ focus is on medically relevant information, though, so the traits tended to be practical: for instance, how prone someone might be to tendon injuries, how muscles would respond to exercise, and how one’s genes might affect blood sugar and cholesterol levels.
Final assessment One thing I discovered from all this testing is that the companies don’t necessarily tell you everything they find in your DNA. Veritas, for instance, sometimes doesn’t report certain information that it doesn’t consider medically relevant. But that decision could have medical consequences.
I learned from 23andMe, for example, that I carry a variant linked to hemochromatosis, a disorder in which excess iron in the blood can build up and damage organs. My variant is unlikely to cause me harm, but it could be a problem for any future children if they also inherited a different harmful variant of the gene from their father. So that’s useful information to have if planning a family. (And indeed, my husband carries this variant, though the odds of us having a child with this disorder are still low.) My Veritas report did not mention the variant. When I checked with the company, Veritas said it chose not to report this variant because of its low likelihood of causing me trouble. But I would prefer to have that information.
Overall, none of these genetic testing companies give you complete information about your health and genetics. Veritas may give you the most bang for your health care dollar, but its report is definitely not as user-friendly as 23andMe’s. Unless you’re a hard-core genetics nerd like me, Genos in its current form could be a frustrating experience.
Before you decide to get your DNA tested for medical reasons, talk to a genetic counselor to see which level of sequencing best suits your needs. If testing uncovers something worrisome, the result should be confirmed by a doctor. Keep in mind that genetics is an inexact science. Someday it will be better. If you can wait for that day, you may have a more satisfying experience. If you just can’t wait, take the results with a grain of salt and keep an open mind. As scientists learn more, interpretations may change.
In 1918, a pandemic of Spanish flu killed as much as 5 percent of the world’s population. A hundred years later, scientists know much more about how to prevent and treat such diseases. But in some ways, the threat of a global outbreak is greater than ever. All it takes is one plane ride for a few localized cases of a disease to become an epidemic.
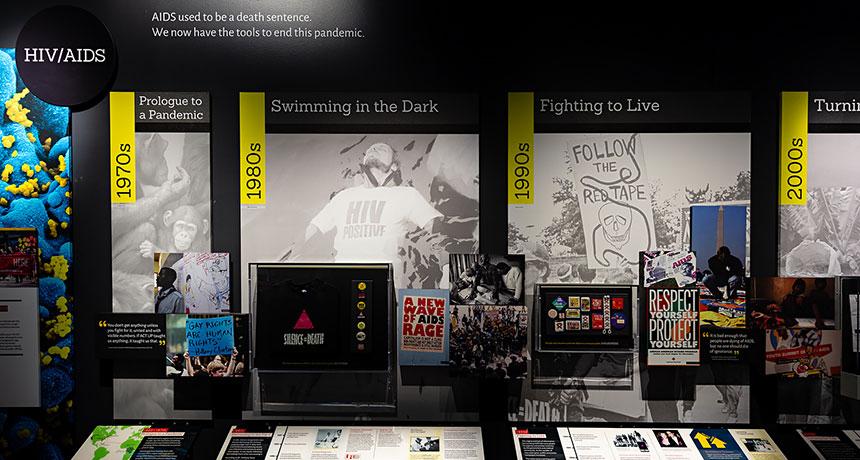
A new exhibit at the Smithsonian National Museum of Natural History in Washington, D.C., traces the way infectious diseases still shape our world. The exhibit, called “Outbreak: Epidemics in a Connected World,” is centered around the concept of One Health — the idea that the health of humans, other animals and the environment are all intertwined, so protecting one requires protecting all (SN: 3/31/18, p. 20). News coverage of disease outbreaks often focuses on the deaths they cause, notes Jonathan Epstein of EcoHealth Alliance, the exhibit’s chief science adviser. One goal of the exhibit, he says, is “to give the public a look at how these things get started.” With that in mind, “Outbreak” highlights a handful of epidemics that have occurred in the last century, using each as a jumping off point to explore different aspects of preventing, tracing, treating and containing infectious diseases. In addition to zeroing in on epidemics that have made international headlines, including Ebola and SARS, the exhibit features lesser-known diseases. Nipah virus, for instance, has infected people in Bangladesh who have drunk sweet date palm sap contaminated by infected bats. Simple preventive measures like encouraging people not to drink the raw sap or to filter it, so far, have prevented the virus from sparking an epidemic.
“Outbreak” is more focused on text and interactive screens than on artifacts, which makes sense given the microscopic subjects. But the exhibit does draw on the Smithsonian’s extensive collections, showcasing arrays of preserved infectious disease vectors, such as ticks and mosquitoes, as well as bat and macaque specimens. As these display cases explain, monitoring the health of animal populations helps researchers put preventive measures in place before emerging infectious diseases can jump to humans. As an entry point for discussing the social side of disease and the stigma that infected people can face, a collection of buttons and signs from AIDS activists recalls the fight for public recognition and government action in the 1980s and ’90s. The content on display might not be a good fit for very young children, but interactive games and activities throughout increase the exhibit’s overall kid appeal. In one game, played on touch screens, players each pick from a variety of roles — such as epidemiologist, wildlife biologist or community worker — and then cooperate to complete tasks that stem the tide of a fictional outbreak. (It’s a good example of the broader message that stopping infectious diseases requires collaboration from many different kinds of experts.)
In case Washington isn’t on your travel agenda, the Smithsonian is translating the content into multiple languages and sharing it with libraries, community centers and other institutions around the world to help them create their own pared-down versions of the exhibit.