COLUMBIA, Mo. — If you find a daddy longlegs in your house, don’t be scared. “Daddy longlegs are actually pretty docile animals when it comes to interacting with humans,” says evolutionary biologist Kasey Fowler-Finn, who studies the arachnids at St. Louis University. Specifically, she studies daddy longlegs sex. She is using this common group of arachnids (they’re not spiders) to explore how mating behaviors can be shaped by evolutionary forces.
Daddy longlegs — which can be found in forests, in leaf litter, on tree trunks and, of course, in your garage in eastern North America — are a group of harvestmen with elongated legs. And like all harvestmen, their second pair of legs, which is used in sensory exploration instead of walking, is particularly long.
But what makes daddy longlegs especially interesting is what happens when they mate. “Most of us just think ‘ew’ when we see them, but they have this really fascinating suite of [mating] behaviors,” Fowler-Finn said July 31 at the 53rd Annual Conference of the Animal Behavior Society. “The same basic stuff happens with all species in the clade, but the details vary quite a bit.”
The mating ritual starts with individuals bumping into each other (scientists don’t yet know how males and females find one another). “Then shortly thereafter, males will attempt to engage the females in what’s called a ‘mating embrace,’” Fowler-Finn said. “They hook their pedipalps [a type of appendage on the front of the arachnid] behind the female’s sensory legs … and then there’s a bunch of back and forth between males and females that varies in duration across species.” Mating can last for 15 seconds in some species, and three to four hours in others. The male then delivers a nuptial gift and his ejaculate, and the pair separates.
There can be a lot of aggression during all of this, with males and females biting each other and even losing legs during mating. And this, too, can vary from species to species. Leiobunum vittatum encounters, for instance, are almost always violent, while L. aldrichi matings are aggressive only about half of the time.
L. aldrichiis one of Fowler-Finn’s favorites. “The male actually grabs the female’s second leg … and then they shake them by one leg,” she said. “And, in fact, this is so particular to the second leg that males who initially grab other legs on the female will continue to search until they find that second leg. So there’s something really cool going on here.” What that might be, though, is a mystery.
Fowler-Finn is still working out whether characteristics of the various daddy longlegs species can predict their mating styles. But she noted that she and her colleagues are finding a lot of variation in behavior not just across species but also by geographic area. She suspects that as she and her team describe these differences, they are going to find evidence for plenty of new species to scare the arachnophobes out there.
Bonobos — chimpanzees’ sister species — don’t get the credit they deserve as tool users.
Bonobos in a sanctuary’s protected forests in the Democratic Republic of Congo crack nuts with stones nearly as well as wild chimps in other parts of Africa do, researchers report online August 26 in the American Journal of Primatology. Wild bonobos have rarely been observed using tools and have never been reported to pound open nuts with stones (SN: 9/19/15, p. 22).
All 18 adult and adolescent bonobos tracked during April and May 2015 cracked oil palm nuts with stones of various sizes that researchers had placed near oil palm trees, says a team led by Johanna Neufuss of the University of Kent in England. Bonobos chose pounding stones well-suited to busting palm oil nutshells. These animals employed 15 grips to hold nut-cracking stones, including 10 grips not previously observed in nonhuman primates.
Genetic surgery is far away for humans — Optimism concerning application of genetic experiments to improve mankind is unwarranted now, a Canadian pediatrician told the Third International Congress of Human Genetics meeting in Chicago…. Although striking and sometimes controversial experiments in genetic surgery have in fact been performed in multicellular systems, he explained, public demand seems likely to outstrip scientific resources for the treatment of many forms of genetic disease. — Science News, September 24, 1966
UPDATE Things are looking up for “genetic surgery.” Gene therapy has been around since the 1980s, but researchers have recently developed more precise gene-editing tools, including one that sent a child’s leukemia into remission in 2015. Scientists are most excited about a molecular scalpel known as CRISPR/Cas9 that cuts and manipulates DNA (SN: 9/3/16, p. 22). Researchers are optimistic about the tool’s potential to treat several diseases, but it may be a while before CRISPR is widely used.
Humankind’s bombs, plastics, chickens and more have altered the planet enough to usher in a new chapter in Earth’s geologic history. That’s the majority opinion of a group of 35 experts tasked with evaluating whether the current human-dominated time span, unofficially dubbed the Anthropocene, deserves a formal place in Earth’s geologic timeline alongside the Eocene and the Pliocene.
In a controversial move, the Anthropocene Working Group has declared that the Anthropocene warrants being a full-blown epoch (not a lesser age), with its start pegged to the post–World War II economic boom and nuclear weapons tests of the late 1940s and early 1950s. The group made these provisional recommendations August 29 at the International Geological Congress in Cape Town, South Africa. If eventually approved by the International Commission on Stratigraphy (ICS) — the gatekeepers of geologic time — and the Executive Committee of the International Union of Geological Sciences, the Anthropocene would usurp the current Holocene Epoch, which has reigned since the end of the last glacial period around 11,700 years ago. The Holocene would become the shortest completed epoch in history, just thousandths the length of the next shortest epoch.
“We’ve left an indelible mark on the Earth,” says Jan Zalasiewicz, a geologist at the University of Leicester in England and convener of the working group. “We now cannot go back to anything that’s ostensibly the same as the Holocene.”
Not all scientists are onboard with the plan. Critics say it’s grounded in politics and pop culture, not science, and that not enough time has passed to put just decades-old changes in context. Any proposal advocating for the Anthropocene will face strong skepticism, says Whitney Autin, a sedimentary geologist at the State University of New York at Brockport. “The idea of amending geologic time carries the same weight as eliminating an amendment to the U.S. Constitution,” he says. To build its case for the new epoch, the working group will spend the next two to three years scouring natural records, such as rocks, mud and tree rings, for evidence that humankind’s impacts have brought about a distinct new phase in the stratigraphic record. The group will then submit a formal proposal for approval.
“We’re leaving physical signals in sediments, in corals, in trees that are going to be long lasting if not permanent,” says Colin Waters, a geologist at the British Geological Survey in Keyworth and a member of the working group. “It’s not just history, it’s geology as well.” And those geologic changes merit official recognition as a new epoch, Waters says.
The goal of the geologic time scale is to label and formalize discrete phases in Earth’s stratigraphic record as a tool for geologists and other scientists. This time scale allows scientists to easily identify, describe and discuss rocks of similar age across the planet.
The term “Anthropocene” has risen in popularity among scientists and the general public in recent years, driven in part by its use in a 2002 article by atmospheric chemist and Nobel laureate Paul Crutzen. The article argued that humans’ exploitation of natural resources has reshaped the planet enough to bring about a new epoch.
While “Anthropocene” now appears in the titles of papers, conference talks and books about everything from climate change to philosophy, those who embrace the term nonetheless disagree on its definition. Some researchers pin the start of the epoch to when humans first started converting forests to farmland thousands of years ago, while others, such as Crutzen, use the start of the Industrial Revolution or the recent acceleration in fossil fuel burning.
The Anthropocene Working Group was convened by the ICS in 2009 to sort out the definition of the Anthropocene and assess whether the time interval should be formally added to the geologic time scale. Among its 35 members, the working group contains an international mix of geologists, climate scientists, archaeologists and other experts.
In January, members of the working group published a review of evidence for the Anthropocene in Science. Pro-Anthropocene arguments come from multiple areas of science, from biology to climate to chemistry, the researchers reported. For instance, humans have introduced species such as the domestic chicken worldwide and driven many others to extinction (SN Online: 8/26/15). Emissions from human activities such as fossil fuel burning have altered Earth’s climate (SN: 4/16/16, p. 22). Manufactured materials such as plastics, aluminum and concrete will remain embedded in the ground as “technofossils.” Fallout from nuclear weapons tests has left a radioactive mark in soil, marine sediments and even ice. These human impacts make the Anthropocene distinct in the stratigraphic record from the Holocene, the researchers concluded.
For the Anthropocene to become official, the working group will have to establish a starting point for the proposed epoch. That can be accomplished by picking a nice round number — the Hadean-Archean switchover is an even 4 billion years ago, for instance — or by linking the starting point to a physical marker in the global sedimentary record, an approach now favored by ICS.
The marker for the start of the Holocene, for instance, is linked to chemical and physical changes in the Greenland ice sheet caused by the warming that brought Earth out of its last bout of glacial growth. Such markers — also called “golden spikes,” similar to the ceremonial spike that marked the union of the first U.S. transcontinental railroad — are chosen for being ubiquitous and consistent throughout the world. Golden spikes are not necessarily important or even relevant to the differences that distinguish geologic time frames, says Stan Finney, a geologist at California State University, Long Beach, and former chair of the ICS. For instance, the Thanetian Age — a 3.2-million-year stretch during the Paleocene Epoch — is marked by just one of many reversals in Earth’s magnetic field.
While a golden spike’s geologic signal may be global, the official physical spike itself is literally a single point in the stratigraphic record somewhere on Earth. (A single point avoids the problem of using multiple points that could end up having different ages, muddling the time boundary.) The golden spike for the Holocene is inside an ice core collected from Greenland and kept chilled in a freezer at the University of Copenhagen.
The need for a golden spike shaped the working group’s Anthropocene proposal, Zalasiewicz says. While phases in human history such as early agriculture and the Industrial Revolution have had profound impacts on the planet, they didn’t have a simultaneous worldwide effect that could be used to mark the start of the new epoch. Had a major volcanic eruption spewed a distinctive layer of ash across the globe near the start of the Industrial Revolution, “it would have been a pretty good candidate,” Zalasiewicz says. Even though the eruption would have had nothing to do with human activity, the ash would have been a ubiquitous and easily identifiable marker for geologists.
Radioactive carbon and plutonium blasted from the ramp up in atmospheric nuclear tests during the 1950s is another story. And the timing is so recent that it opens up many new places to hunt for the proposed epoch’s golden spike, including in living organisms such as trees and corals. “We’re a bit like confused kids wandering around an enormous sweetshop wondering how we’re going to choose,” Zalasiewicz says.
Even if the group finds a golden spike, its proposal will face criticism from scientists who contend that the Anthropocene doesn’t warrant its own epoch. Radioactive fallout “is a widespread marker that qualifies for the rules that they need to follow to make a recommendation,” says William Ruddiman, a professor emeritus at the University of Virginia in Charlottesville, “but that doesn’t mean that it’s right, or that it makes sense.”
Not enough time has passed since the proposed start date of the Anthropocene to have enough perspective to put the observed changes in the sedimentary record in proper context, Autin says. “A lot of stratigraphers would say that maybe in thousands or millions of years there will be a distinctive demarcation in the rock record at this point in time, but right now it’s a proposal that’s premature.”
Placing the boundary so recently is “dubious, to say the least,” agrees Mike Walker, a professor emeritus at the University of Wales Trinity Saint David who helped establish the golden spike that represents the start of the Holocene. Divisions of geologic time “should have a utility for geoscientists, archaeologists, anthropologists, et cetera,” he says. “I see little of value to the wider science community in an epoch boundary at A.D. 1950.”
The formalization of the Anthropocene is not just scientifically motivated, but also driven by a desire to highlight humankind’s impact on the environment, suggests Lucy Edwards, a geologist with the U.S. Geological Survey in Reston, Va. “It’s a meme,” she says. “The thinking is that if you have a concept and you give it a new word, it carries more weight.”
The motivation behind the newly announced proposal isn’t overly focused on humankind being to blame for recent changes, Zalasiewicz responds. “If we had all the same changes, but caused by something else, like volcanoes or a meteorite or my cat, then it would be just as significant.”
More time isn’t needed to recognize that modern sediments are unique, he adds. After all, he says, if humans had been around 50 years after the environmental catastrophe that wiped out the dinosaurs about 66 million years ago, they would have clearly seen that Earth’s environment and ecology had permanently changed.
ORLANDO, Fla. — When sex chromosomes among common pill bugs go bad from disuse, borrowed bacterial DNA comes to the rescue. Certain pill bugs grow up female because of sex chromosomes cobbled together with genes that jumped from the bacteria.
Genetic analysis traces this female-maker DNA to Wolbachia bacteria, Richard Cordaux, based at the University of Poitiers with France’s scientific research center CNRS, announced September 29 at the International Congress of Entomology.
Various kinds of Wolbachia infect many arthropods, spreading from mother to offspring and often biasing their hosts’ sex ratios toward females (and thus creating even more female offspring). In the common pill bug (Armadillidium vulgare), Wolbachia can favor female development in two ways. Just by bacterial infection without any gene transfer, bacteria passed down to eggs can make genetic males develop into functional females. Generations of Wolbachia infections determining sex let these pill bugs’ now-obsolete female-making genes degenerate. Which makes it very strange that certain populations of pill bugs with no current Wolbachia infection still produce abundant females. That’s where Cordaux and Poitier colleague Clément Gilbert have demonstrated a second way that Wolbachia makes lady pill bugs — by donating DNA directly to the pill bug genes. The researchers, who share an interest in sex determination, have built a case that Wolbachia inserted feminizing genes into pill bug chromosomes. The bacterial genes thus created a new sex chromosome.
“Incredible,” said Steve Perlman after hearing the talk, not in disbelief but in wonder at the biology. Perlman, of the University of Victoria in Canada, studies symbiosis and parasitism and says this new example of far-flung gene transfer is part of “a big thing in the field now.” Such transfers provide exotic genetic variation that fuels evolutionary processes. Audience members Ellen Martinson and Vincent Martinson, both of the University of Rochester in New York, were themselves coauthors of a 2016 paper describing microsporidian fungus DNA that has become a venom gene in some wasps.
To the bafflement of birders, yellow-shafted flickers (Colaptes auratus auratus) sometimes sport red or orange wing feathers.
Scientists have suggested that the birds, which inhabit eastern North America, might be products of genetic variation affecting the carotenoid pigments that produce their flight-feather colors. Alternatively, the birds might be hybrids from mixing with a subspecies that lives in the west, red-shafted flickers (Colaptes auratus cafer). Despite decades of study, no clear-cut explanation has emerged.
It turns out that diet may be to blame. Jocelyn Hudon of the Royal Alberta Museum in Canada and her colleagues tested the red flight feathers from two yellow-shafted flickers and found traces of rhodoxanthin, a deep red pigment found in plants, and a potential metabolite. This suggests that the birds’ bodies break down rhodoxanthin — a clue that the pigment enters the body through food. Spectral and biochemical tests of feathers from museum collections also point to rhodoxanthin and suggest that the pigment may mess with yellow carotenoid production as well.
Yellow-shafted flickers probably pick up the red pigment when they eat berries from invasive honeysuckle plants, which contain the ruby pigment and produce similar red hues in other birds, the researchers write October 12 in The Auk. The plants also happen to produce berries just around the time that flickers molt their flight feathers.
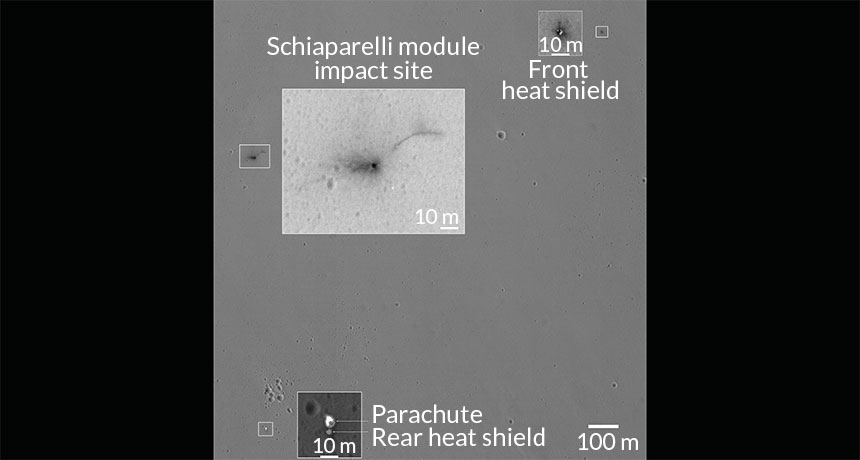
The Schiaparelli Mars lander, missing in action since its October 19 descent, dinged the surface of the Red Planet. A black spot framed by dark rays of debris mark the lander’s final resting place, the European Space Agency reports online October 27. Its parachute, still attached to the rear heat shield, lies about 1.4 kilometers to the south, new images from the Mars Reconnaissance Orbiter show. The front heat shield, ejected about four minutes into the descent, sits roughly 1.4 kilometers to the east of the impact site.
Radio contact with Schiaparelli was lost about 50 seconds before its planned landing. Early analysis of data from the lander indicate that the parachute was jettisoned prematurely and that the landing rockets shut off just a few seconds after igniting. Engineers with ESA’s ExoMars mission are still analyzing that data to understand what went wrong.
Below most volcanoes, Earth packs some serious deep heat. Mount St. Helens is a standout exception, suggests a new study. Cold rock lurks under this active Washington volcano.
Using data from a seismic survey (that included setting off 23 explosions around the volcano), Steven Hansen, a geophysicist at the University of New Mexico, peeked 40 kilometers under Mount St. Helens. That’s where the Juan de Fuca tectonic plate releases fluids due to intense heat and pressure as it descends beneath the North American plate. Those fluids rise and trigger melting in the rock above, fueling an arc of volcanoes that line up like lights on a runway. All except for Mount St. Helens, which stands apart about 50 kilometers to the west. Still, Hansen and colleagues expected to see a heat source under Mount St. Helens, as seen at other volcanoes. Instead, thermal modeling revealed a wedge of a rock called serpentinite that’s too cool to be a volcano’s source of heat, the researchers report November 1 in Nature Communications. “This hasn’t really been seen below any active arc volcanoes before,” Hansen says.
This odd discovery helps show what the local crust-mantle boundary looks like, but raises another burning question: Where is Mount St. Helens’ heat source? Somewhere to the east, suggests Hansen. Exactly where, or how it reaches the volcano, remains a cold case.
Editor’s Note: this article was revised on January 4, 2017, to note how the Juan de Fuca tectonic plate fuels the chain of volcanoes.
Global emissions of carbon dioxide won’t increase much in 2016 despite overall economic growth, newly released bookkeeping suggests. The result marks a three-year-long plateau in the amount of CO2 released by human activities, scientists from the Global Carbon Project report November 14 in Earth System Science Data.
The group’s projected rise in CO2 emissions of 0.2 percent for 2016 is far lower than the rapid emissions growth of around 2.3 percent annually on average from 2004 through 2013. Emissions increased by about 0.7 percent in 2014 over the previous year and remained largely flat in 2015.
China is largely responsible for the emissions slowdown, the researchers write. The country is the world’s largest carbon dioxide emitter and is projected to reduce its CO2 emissions by 0.5 percent this year.
SAN ANTONIO — A roughly 3,000-year-old cemetery on Israel’s coast is providing an unprecedented look at burial practices of the Philistines, a mysterious population known from the Old Testament for having battled the Israelites.
Work at the Ashkelon cemetery from 2013 to 2016 has uncovered remains of at least 227 individuals, ranging from infants to older adults. Only a small section of the cemetery has been explored. Archaeologist and excavation director Adam Aja of the Harvard Semitic Museum estimates that approximately 1,200 people were interred there over a span of about 100 years. “For the first time, we have found a formal Philistine cemetery,” Aja said November 18 at the annual meeting of the American Schools of Oriental Research. Aja and his colleagues first announced having found the Philistine graveyard on July 10. He was among several researchers to present their latest findings about the cemetery at the meeting.
Despite the new discoveries, the geographic origins of the Philistines remain unknown, Aja said. It’s also unclear how early Philistines reached the Middle East or how much their culture changed by the time they started burying their dead at Ashkelon.
Philistine burial practices have been discussed and debated for about a century. Other ancient Philistine sites in Israel, also identified in ancient texts, have yielded individual graves and small-scale burial grounds.
At Ashkelon, the dead were interred in several ways. Most individuals were placed in shallow pits, often with pairs of jugs or storage containers near the bodies. Some pits contained a person’s remains that had been buried on top of one or more previously interred bodies. Bronze earrings, bracelets, rings and other jewelry adorn most skeletons of children and women. Several pit graves of male skeletons include ornamental beads or engraved stones.
One grave holds a set of iron arrows near a man’s hip. A quiver probably once held the arrows at the man’s side, Aja suggested. Researchers also uncovered ashes and bone fragments from six human cremations in sealed jars placed in pit graves.
At least eight stone burial chambers capped with stone slabs were also found. The largest chamber held skeletons of 23 individuals. These burial chambers were aligned in three rows that ran parallel to the coast, Aja said.
Tapered storage jars found in pit graves and burial chambers were influenced by pottery of the Canaanites, a nearby population along the Mediterranean coast, said team member Janling Fu of Harvard University.
Fu suspects the excavation is located at the cemetery’s edge. Considerable space between some burials suggests denser clusters of grave sites lie nearby, he proposed, raising the prospect of learning much more about how the Philistines treated their dead.
Although the excavation is in its early stages, it’s clear that Philistines buried at Ashkelon show signs of physiological stress, reported bioarchaeologist and team member Sherry Fox of Eastern Michigan University in Ypsilanti. Many individuals’ teeth have signs of growth interruptions caused by fever, malnutrition or a range of possible biological disorders, she said.
Relatively short average heights for people buried at Ashkelon — about 5 feet, 1 inch for men and 4 feet, 10 inches for women — also fit a scenario of biological stress, Fox said. Short stature and minimal height differences between men and women occur with population-wide stresses such as malnutrition, she said.
The Philistines were a famously combative crowd. Archaeologist Eric Meyers of Duke University, who was not a member of the Ashkelon team, wondered if at least some of those buried at Ashkelon had been killed in battles or fights. But no head injuries or other skeletal signs of violent encounters appeared among the dead at Ashkelon, Fox said. Neither did any skeletons contain evidence of tumors or cancers.
If DNA can be extracted from the Ashkelon skeletons, scientists may get a glimpse of where the Philistines originally came from. Evolutionary geneticist Johannes Krause of the Max Planck Institute for the Science of Human History in Jena, Germany, is currently directing efforts to retrieve genetic sequences from the Ashkelon bones.