Chemical transformations in minerals deep beneath the seafloor could explain why Indonesia’s 2004 mega-earthquake was unexpectedly destructive, researchers report in the May 26 Science.
The magnitude 9.2 quake and the tsunami that it triggered killed more than 250,000 people, flattened villages, and swept homes out to sea across Southeast Asia. It was one of the deadliest tsunamis in recorded history.
“It raised a whole bunch of questions, because that wasn’t a place in the world where we thought a magnitude 9 earthquake would occur,” says study coauthor Brandon Dugan, a geophysicist at the Colorado School of Mines in Golden.
The thick but stable layer of sediment where tectonic plates meet off the coast of the Indonesian island of Sumatra should have limited the power of an earthquake, seismologists had predicted. But instead, this quake was the third-strongest on record worldwide. Dugan spent two months aboard a boat with 30 other scientists collaborating through the International Ocean Discovery Program. The researchers drilled down 1,500 meters below the seafloor in two places off the coast of Sumatra, extracting narrow cylinders of sediment. This sediment is very slowly moving toward the fault where the 2004 earthquake occurred — a zone where one massive tectonic plate slides over another, pushing that plate downward.
Analyzing how sediment changes with depth can give scientists a snapshot of the geological processes at play near the fault zone.
In particular, deep down, the researchers identified a layer of sediment where the water had a lower salinity than the water in the sediment above or below. Since seawater seeping into the sediment would be salty, the evidence of freshwater suggests that the water must have instead been released from within minerals in the sediment.
For tens of millions of years, Dugan proposes, minerals sat on the seafloor taking in water — baking it into their crystal structure. Then, more sediment settled on top. It got toasty under such a thick blanket of sediment, heating up the minerals beneath. The temperature increase triggered a chemical transformation within the sediment, pushing water out of the mineral crystals and into tiny pores between the grains. The sediment sampled in this study is still dehydrating. By the time any of it reaches the plate boundary, Dugan says, it’ll be buried under kilometers of more sediment and will probably be completely dehydrated.
At first, the liberated water would have softened the material, actually decreasing the risk of a big earthquake by allowing it to absorb more force, Dugan says. As the sediment got closer to the fault over millions of years, though, the water flowed away, leaving it brittle and unstable — the perfect setup for a mega-quake.
The timing of this sediment dehydration process can make or break a quake. Had the sediment near the fault been in a softened state when the quake struck in 2004, the tremor might not have been as deadly, Dugan says. But since enough time had passed for it to become brittle again, the tectonic plates were able to rapidly slip past each other for a much greater distance during the quake. That massive motion displaced the seafloor itself, setting a tsunami into motion. “It’s really the tsunamis from these earthquakes that prove to be the deadliest and most dangerous,” says Roland Bürgmann, a seismologist at the University of California, Berkeley who wasn’t part of the study. And quakes that displace the seafloor are far more likely to trigger tsunamis.
The findings could apply to other faults with similarly thick sediment, such as the Cascadia Subduction Zone in the Pacific Northwest, suggests study coauthor Andre Hüpers, a geophysicist at the University of Bremen in Germany.
But more evidence is needed before applying such analysis to faults beyond this one, says Bürgmann. The argument for what happened along the Sumatran fault is compelling, he says. “But nonetheless, it’s only one data point. It doesn’t yet make for a pattern.”
The first thing you’ll notice is the noise. Monitors beep steadily, relentlessly, ready to sound a car-alarm blare if a baby is in trouble.
The air has an astringent odor — not clean exactly, but reminiscent of an operating room (there’s one next door). Ceiling lights shine fluorescent white. Half are off, but glare from the monitors throws out extra light. It’s midday on a Friday, but it’ll be just as bright at midnight.
Here on the fourth floor of Yale New Haven Children’s Hospital, 10 tiny beds hold 10 tiny infants, each with Band-Aid–like patches stuck to their bodies to continuously monitor health. Between beds, nurses squeeze through narrow aisles crammed with folding chairs and plastic incubators. This space, one of five in the hospital’s neonatal intensive care unit, has the people and equipment needed to keep sick babies alive — heart rate monitors, oxygen tanks, IV poles to deliver medications. Until recently, Yale’s NICU and hundreds like it across the country were considered the place to be for newborns withdrawing from opioid drugs. But now, as the number of drug-dependent babies surges, doctors here and elsewhere are searching for better options.
“We’re really focused on trying to get these kids out of the NICU,” says Yale pediatrician Matthew Grossman. “We’re looking at moms and the dads as the first line of treatment.”
The nationwide rate of babies withdrawing from opioids has soared — up nearly 400 percent from 2000 to 2012. The booming numbers are the bleak by-product of the United States’ ongoing battle with the drugs: Sales of prescription opioid pain relievers alone quadrupled from 1999 to 2010, and overdose deaths tripled from 2000 to 2014. When pregnant women use opioids, the drugs pass from bloodstream to baby. After exposure in the womb to Vicodin, methadone or heroin, for example, babies can become dependent. At birth, when the drug flow stops, babies can go through agonizing withdrawal — body shakes, intestinal problems, constant crying. The condition is known as neonatal abstinence syndrome, or NAS. But there’s no clear consensus on how to care for these struggling babies, Grossman says. Usually they’re whisked off to the NICU and treated with opioids. The drugs ease symptoms, but they prolong exposure to “really powerful and potentially dangerous medications,” he says.
At Yale, NAS babies used to spend weeks in the NICU — they still do in many U.S. hospitals. But in the last few years, Grossman and others have begun to question this method of care. Infants suffering from opioid withdrawal might actually do better back in parents’ arms, away from the high-tech hubbub. Comfort is key. Quiet, dark environments, swaddling, breastfeeding, rocking and holding, no unnecessary tests — it’s baby care 101.
That’s hard to do in the busy, loud NICU, says Grossman. Plus, there’s no place for parents to stay. They can visit, perched on folding chairs wedged between beds, says Yale pediatrician Rachel Osborn, but moms and dads “often feel like they’re extraneous and in the way.”
Faced with these and other obstacles, Grossman, Osborn and others are radically redefining their methods. They’re examining traditional practices, testing new ideas and getting back to basics. The results have been dramatic.
“We’re treating the families with respect and the babies like babies,” Grossman says. The parents have everything the baby needs, he says. “It’s not a whole lot more complicated than that.” State of alarm Maine, Vermont and West Virginia reported the highest rates of neonatal abstinence syndrome, opioid withdrawal linked to maternal drug use. Maine, Maryland, Massachusetts and Rhode Island rates are from 2012; the rest are 2013.
Click or tap the map below to learn more. Tough going Families today are much more likely to deal with opioid use — and its consequences for newborns — than they were a decade ago.
In 2004, NAS rates were consistently low across the country: For every 1,000 babies born, roughly one was diagnosed with NAS. By 2013, when pediatrician Nicole Villapiano and colleagues examined rural versus urban data, rates were up across the board. But rural areas had been hit the hardest, with nearly 8 per 1,000 babies diagnosed with NAS, the researchers reported in February in JAMA Pediatrics.
In an urban hospital near Rhode Island’s Providence River, Villapiano witnessed infant opioid withdrawal firsthand. She was first assigned to the newborn nursery service at Women and Infants Hospital in Providence in 2011. “I imagined it’d be a joyful time, seeing babies going off with their families, having wonderful lives.”
Reality quickly dashed that hopeful picture. On any given day, she might see several babies at a time struggling with withdrawal. “These children were miserable,” says Villapiano, now at the University of Michigan in Ann Arbor. “Their cries were persistent and their irritability was profound.”
NAS isn’t easy to define. Babies suffer a wide range of symptoms. They’re sweating, shaking, stiff. Stools are loose, eating and sleeping are difficult, and crankiness is common. Babies with NAS can also have breathing problems, seizures and low birth weights.
The syndrome was first described in heroin-exposed infants. Scientists now know that all sorts of opioids used during pregnancy can trigger the condition, including “maintenance” drugs like methadone or buprenorphine used to treat opioid addiction, and even painkillers commonly prescribed during pregnancy, such as codeine and hydrocodone.
Not all infants exposed to opioids in utero go through withdrawal — and exactly what conditions lead to NAS is still unclear. The particular opioid and how much a pregnant woman uses, whether she takes certain antidepressants and even the number of cigarettes she smokes per day all seem to factor in, Stephen Patrick of Vanderbilt University in Nashville and colleagues reported in Pediatrics in 2015. A nonsmoking woman on oxycodone for a few weeks, for example, might have roughly a 1 percent chance of delivering a baby with NAS. For a pack-a-day smoker on antidepressants and buprenorphine for six months, the risk could be more than 30 percent.
Because opioids are such a broad family of addictive drugs, opioid-using moms don’t fit neatly into one category, says Ju Lee Oei, a neonatologist at the University of New South Wales in Sydney. “We need to be aware that Mrs. Smith down the road who’s getting a bit of codeine for her back pain could have a baby with NAS,” Oei says. Some women give birth to NAS babies while recovering from opioid addiction — even though they’re doing everything doctors advise, says pediatrician Alison Holmes of Children’s Hospital at Dartmouth-Hitchcock in Lebanon, N.H.
“Sometimes people think, ‘Oh, these mothers are such horrible addicts,’ ” Holmes says. But a lot of the time, “they’re staying on their methadone, they’re staying on their buprenorphine, they’re keeping symptoms under control — but their babies are still going to withdraw.”
No one knows exactly what opioid exposure does to fetal brains, or how these kids will fare in the future. Certain brain regions may not grow correctly, previous studies have suggested. Children can also have vision trouble and may develop behavior and attention problems. One long-term Australian study published in February linked a diagnosis of NAS with poor academic performance — all the way up to age 12 or 13.
Whether that’s caused by NAS is hard to say, says Oei, a coauthor of the study. Poverty, poor childhood nutrition and prenatal exposure to alcohol or other drugs could also come into play. But the results are a red flag for all those newly diagnosed babies. “You expect your baby to go to school and get good grades,” Oei says. But from as early as third grade, “these kids don’t seem to be able to do that.”
Still, research on NAS outcomes and potential treatments remains full of gaps, a 2015 report from the U.S. Government Accountability Office found. And there’s no nationally accepted treatment protocol for NAS. “Everyone’s doing it their own way,” says Scott Wexelblatt, a pediatrician at Cincinnati Children’s Hospital Medical Center.
Time for a change The traditional way to assess NAS was published more than 40 years ago by neonatologist Loretta Finnegan, now at the College on Problems of Drug Dependence in Philadelphia. Every four to eight hours, sometimes more frequently, nurses evaluate symptoms using a detailed scoring list: the Finnegan Neonatal Abstinence Scoring System. Hit a certain score, and doctors will start up the withdrawal-easing opioids, typically morphine or methadone. But there’s a push and pull between managing withdrawal and dosing babies with more drugs, Wexelblatt says. “We don’t want to expose babies to opioids unless we really need to.”
Care of NAS babies varies widely in hospitals across the United States, according to a study in the May–June Academic Pediatrics. Some newborns may be getting too much opioids. To see if standardizing care could help infants get off the drugs faster, Wexelblatt and colleagues trained nurses on Finnegan scoring and outlined a detailed protocol for weaning.
That simple step made a big difference. Hospitals that adopted the protocol cut infant stays from an average of 31.6 days before the intervention to 23.7 days afterward, Wexelblatt’s team reported in 2015 in Pediatrics. Duration of opioid treatment dropped as well. By 2016, hospital stays were down to 20 days, he says.
Now, 54 hospitals — almost all delivery hospitals in Ohio — use the weaning protocol, Wexelblatt says. The team has since refined its methods, focusing on family support and nonmedication options for care, like swaddling and breastfeeding. And as of 2013, every delivering mom in the Cincinnati region gets urine-tested for opioids upon admission so that care can start early, if needed. Ohio’s strategy is paying off: Doctors are using fewer opioids to treat NAS babies and the infants are getting out of the hospital faster too, early results suggest.
Researchers at Yale and Dartmouth-Hitchcock have also taken a hard look at the hospitals’ methods, starting with the Finnegan scoring system. Some aspects just didn’t make sense, Holmes and colleagues reported last June in Pediatrics. Nurses sometimes woke sleeping babies or removed them from family members’ arms for scoring, and they gave hungry babies points for crying.
“We said, ‘This is crazy,’ ” Holmes remembers. It makes more sense to just score the babies after they eat and while they’re being held. That way, she says, nurses might be able to sift the actual signs of withdrawal from the normal whines and wails of a hungry or tired baby.
Grossman and colleagues at Yale were skeptical too. Finnegan’s system looks for warning signs like vomiting and fever, but also gives points for sneezing and yawning. The final score guides doctors’ decision to dial meds up or down. “Is it truly best to give morphine to an infant who yawned 4 times instead of 3, as the [scoring system] guides us to do?” they asked in a Hospital Pediatrics commentary in February.
Grossman scoured the scientific literature, searching for clues to improve treatment. But research results bounced all over the place. “We ended up questioning everything,” he says. “It turned out there wasn’t really a good answer for anything we were doing.” Family first Around the same time Grossman was digging into research on opioid withdrawal in newborns, he had his first child, who screamed constantly. “I’m pacing in the middle of the night, thinking, if this was an NAS baby, he’d be on medication immediately.”
Instead, Grossman paced and rocked and held his son — all of the tricks parents use to soothe a cranky newborn. As he found ways to settle the baby, he thought, what if NAS babies needed something similar?
The idea jibed with his experiences at the hospital. Sometimes withdrawing infants would do great for days—their moms were there, and Finnegan scores stayed low. But if moms had to leave, babies would backslide, and scores would rocket up again. “Do these kids need more mom or more meds?” Grossman and colleagues wondered. “We started to think, ‘Well, maybe it’s more mom.’ ”
At Dartmouth-Hitchcock, Holmes and her crew were coming up with their own ideas. The team stopped interpreting Finnegan scores so rigidly, for one. But their biggest change was keeping mothers and babies together, 24-7. It’s called “rooming-in,” and previous studies in Canada and other countries had suggested it might ease babies’ transition from the womb to the world. “What withdrawing babies need is a calm, quiet, dark place where they can be held by a caring individual,” Holmes says. Her team focused on involving moms and families (and even volunteer cuddlers), and the hunch paid off. From 2012 to 2015, the average length of stay for morphine-treated NAS babies dropped from 16.9 days to 12.3 days. The fraction of babies given morphine plummeted too, from 46 percent to 27 percent. Now, two years later, that number has fallen even further — to just 20 percent, she says.
Holmes says her own kids joke about her work: “Babies like their mothers—surprise, surprise! What a discovery!” She laughs, and then adds, “They’re kind of right.”
Grossman’s team at Yale has pushed the family-focused approach even further. “Our mind-set is rooming-in on steroids,” he says. For NAS, parental care is considered more important—and more effective—than medication. Doctors ask parents: “How do we get you here or dad here or grandma here?” Grossman says. “Because that’s what your baby needs.”
His team rolled in other ideas too, like fortifying formula and pumped breast milk with extra calories. And hospital personnel stopped using Finnegan scores to guide medication dosing. Today, they base assessments on three simple parameters: whether an infant can eat, sleep and be consoled.
The patient rooms where parents can bunk with their babies are a world apart from the NICU. One room at Yale has a couch that converts into a bed and ceiling tiles with pictures of Elmo and Tweety Bird. Monitors are muted, nothing beeps incessantly and natural light pours in from the window. There’s plenty of space for parents to walk around and tend to their baby. In these rooms, “it feels like the parent is a necessary part of the care team,” Yale’s Osborn says.
In 2016, babies with NAS stayed in the Yale hospital just 5.9 days — a cliff dive compared with the 2008–2010 average of 22.4 days, Grossman, Osborn and colleagues reported online May 18 in Pediatrics. Even more staggering is the fraction of these babies treated with morphine: just 14 percent in 2016, down from 98 percent in 2008–2010. Taking the plunge From 2008 to 2016, the proportion of opioid-withdrawing infants treated with morphine at Yale New Haven Children’s Hospital dropped from 98 percent to 14 percent, a drastic reduction in the number of babies given the medication.
Click or tap the graph below to learn more.
Yale’s approach basically comes down to common sense, Grossman says: a quiet room, lots of holding, feeding when hungry and simply keeping babies with mom and dad. “It’s not rocket science,” he says. Medication became more of a plan B.
Still, other doctors looking to transform NAS treatment may run into barriers. Not all U.S. hospitals are set up like Dartmouth-Hitchcock or Yale New Haven, Wexelblatt says. There’s not always room for mom to stay with her baby once she’s released. And universal drug testing of moms won’t work everywhere, he warns. In Tennessee, a law passed in 2014 allowed new mothers to be prosecuted for using illegal drugs while pregnant if the newborn was harmed. The law expired last July, but such legislation drives women away from medical care, Wexelblatt says.
It could be that the best care for babies begins with care and compassion for moms. Rather than blame mothers, Holmes says, “We need to do as much as we can to support them in being good parents.”
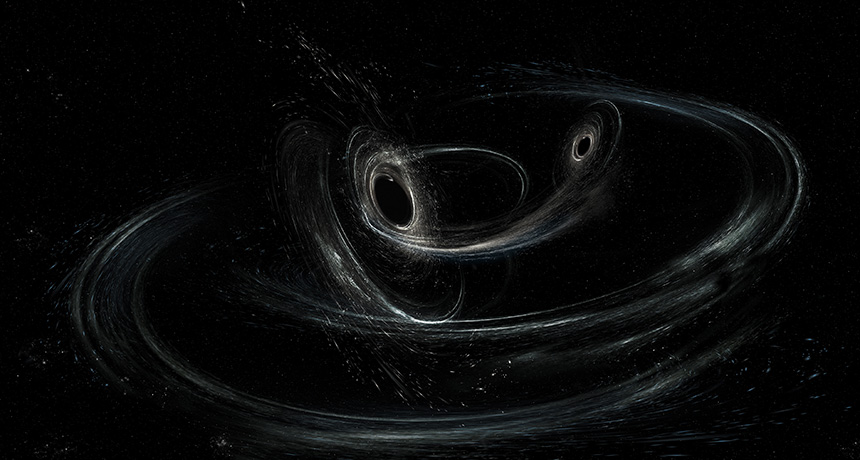
Gravitational waves are providing new hints about how black holes get their kicks.
The Advanced Laser Interferometer Gravitational-Wave Observatory’s detection of spacetime ripples from two merging black holes on December 26, 2015, indicated that one black hole was spinning like a tilted top as it orbited with its companion (SN: 7/9/16, p. 8). That off-kilter spin could mean that the stellar explosion that produced the black hole gave it a strong kick, physicist Richard O’Shaughnessy and colleagues report in a paper in press in Physical Review Letters.
Scientists aren’t sure how black holes like those detected by LIGO pair up (SN Online: 6/19/16). Two neighboring stars may have obliterated themselves in a pair of explosions called supernovas, producing two black holes. But that scenario should lead to black holes that spin in the same plane as their orbit. It would take a sizeable jolt from the supernova, of about 50 kilometers per second, to account for the cockeyed spin, the researchers conclude.
Computer simulations of supernovas predict smaller black hole boosts, making for a cosmological conundrum. “This will be a serious challenge for supernova modelers to explain,” O’Shaughnessy, of the Rochester Institute of Technology in New York, said June 5 in a news conference in Austin, Texas, at a meeting of the American Astronomical Society.
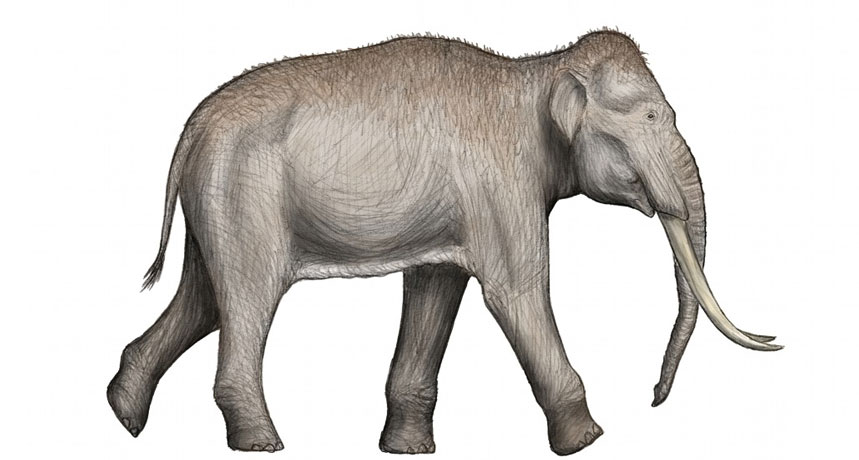
Fossil DNA may be rewriting the history of elephant evolution.
The first genetic analysis of DNA from fossils of straight-tusked elephants reveals that the extinct animals most closely resembled modern African forest elephants. This suggests that straight-tusked elephants were part of the African, not Asian, elephant lineage, scientists report online June 6 in eLife.
Straight-tusked elephants roamed Europe and Asia until about 30,000 years ago. Much like modern Asian elephants, they sported high foreheads and double-domed skulls. These features convinced scientists for decades that straight-tusked and Asian elephants were sister species, says Adrian Lister, a paleobiologist at the Natural History Museum in London who was not involved in the study. For the new study, researchers extracted and decoded DNA from the bones of four straight-tusked elephants found in Germany. The fossils ranged from around 120,000 to 240,000 years old. The genetic material in most fossils more than 100,000 years old is too decayed to analyze. But the elephant fossils were unearthed in a lake basin and a quarry, where the bones would have been quickly covered with sediment that preserved them, says study author Michael Hofreiter of the University of Potsdam in Germany.
Hofreiter’s team compared the ancient animals’ DNA with the genomes of the three living elephant species — Asian, African savanna and African forest — and found that straight-tusked genetics were most similar to African forest elephants.
When the researchers told elephant experts what they’d found, “Everybody was like, ‘This can’t possibly be true!’” says study coauthor Beth Shapiro of the University of California, Santa Cruz. “Then it gradually became, ‘Oh yeah, I see.… The way we’ve been thinking about this is wrong.’”
If straight-tusked elephants were closely related to African forest elephants, then the African lineage wasn’t confined to Africa — where all elephant species originated — as paleontologists previously thought. It also raises questions about why straight-tusked elephants bore so little resemblance to today’s African elephants, which have low foreheads and single-domed skulls. Accounting for this new finding may not be as simple as moving one branch on the elephant family tree, Lister says. It’s possible that straight-tusked elephants really were a sister species of Asian elephants, but they exhibit genetic similarities to African forest elephants from interbreeding before the straight-tusked species left Africa.
It’s also possible that a common ancestor of Asian, African and straight-tusked elephants had particular genetic traits that were, for some reason, only retained by African and straight-tusked elephants, he says.
Lister and colleagues are now reexamining data on straight-tusked skeletons to reconcile the species’ skeletal features with the new information on their DNA. “I will feel most comfortable if we can understand these genetic relationships in terms of the [physical] differences between all these species,” he says. “Then we’ll have a complete story.”
When we brought our first baby home from the hospital, our pediatrician advised us to have her sleep in our room. We put our tiny new roommate in a crib near our bed (though other containers that were flat, firm and free of blankets, pillows or stuffed animals would have worked, too).
The advice aims to reduce the risk of sleep-related deaths, including sudden infant death syndrome, or SIDS. Studies suggest that in their first year of life, babies who bunk with their parents (but not in the same bed) are less likely to die from SIDS than babies who sleep in their own room. The reasons aren’t clear, but scientists suspect it has to do with lighter sleep: Babies who sleep near parents might more readily wake themselves up and avoid the deep sleep that’s a risk factor for SIDS.
That’s an important reason to keep babies close. Room sharing also makes sense from a logistical standpoint. Middle of the night feedings and diaper changes are easier when there’s less distance between you and the babe.
But babies get older. They start snoring a little louder and eating less frequently, and it’s quite natural to wonder how long this room sharing should last. That’s a question without a great answer. In November 2016, the American Academy of Pediatrics task force on SIDS updated its sleep guidelines. The earlier recommendation was that babies ought to sleep in parents’ bedrooms for an entire year. The new suggestion softens that a bit to say infants should be there for “ideally for the first year of life, but at least for the first 6 months.”
Rachel Moon, a SIDS expert at the University of Virginia in Charlottesville who helped write the revised AAP guidelines, says that the update “gives parents a little more latitude after the first 6 months.” The vast majority of SIDS deaths happen in the first six months of life, but the studies that have found benefits for room sharing lumped together data from the entire first year. That makes it hard to say how protective room sharing is for babies between 6 and 12 months of age.
But a new study raises a reason why babies ought to get evicted before their first birthday: They may get more sleep at night in their own rooms. Babies who were sleeping in their own rooms at ages 4 or 9 months got more nighttime sleep than babies the same ages who roomed with parents, researchers reported online June 5 in Pediatrics.
The team asked hundreds of mothers to take sleep surveys when their children were 4, 9, 12 and 30 months old. Some of the 230 children slept in their own rooms when they were younger than 4 months, others moved to their own rooms between 4 and 9 months, and the rest were still sharing their parents’ rooms at 9 months. At 9 months, babies who had been sleeping alone since 4 months of age slept an average of 40 minutes more than room sharers. The researchers found no differences in sleep duration between the groups of babies at age 12 months. By 30 months of age, though, children who had been sleeping in their own rooms by either 4 or 9 months of age slept on average 45 minutes longer at night than children who had been sharing their parents’ rooms at 9 months. (Important caveat: At 30 months, total daily sleep time didn’t differ between the groups. The former room sharers were making up for missed nighttime sleep with naps.)
Parents who want their babies age 6 months and older to sleep in their own room ought to be encouraged to make the move, says study coauthor Ian Paul, a pediatrician at Penn State. “The guidelines should reflect data, not opinion,” Paul says.
He suspects that sharing a bedroom with babies interferes with everyone’s sleep because normal nocturnal rustlings turn into full-blown wake-ups. Babies and adults alike experience brief arousals during sleep. But when parents are right next to babies, they’re more likely to respond to their children’s brief arousals, which then wakes the baby up more. “This then sets up the expectation from the baby that these arousals will be met with a parent reaction, causing a bad cycle to develop,” he says.
There was another difference that turned up between the two groups of babies. Babies who roomed with parents were four times more likely to be moved into their parents’ beds at some point during the night than babies who slept in their own rooms. Bed sharing is a big risk factor for sleep-related infant deaths.
But Moon cautions that the Pediatrics study is preliminary, and doesn’t warrant a change in the AAP guidelines. She and coauthors point out in an accompanying commentary that other factors might be behind the difference in sleep between the two groups of babies. For instance, babies who slept in their own room were more likely to have consistent bedtime routines, be put to bed drowsy but awake, and have bedtimes of 8 p.m. or earlier. Those are all signs of good “sleep hygiene” for babies, and might be contributing to the longer sleep times. “We know that consistent bedtime routine and consistent bedtime are very important in terms of sleep quality in children,” Moon says. “They could very well make a difference.”
So that’s where we are. Some things are clear, like putting your baby to sleep on her back on a flat, firm surface clear of objects and having your baby nearby during the first six months. But other decisions come with skimpier science, and whether to evict your 6-month-old is one of them. Because science can take you only so far, it may just come down to the snoring, stirring and sleep deprivation.
BOSTON — Some aspects of speech are as Southern as pecan pie. Consider the vowel shift that makes the word pie sound more like “pah.” While that pronunciation is found from Florida to Texas, a new study reveals a surprising diversity in Southern vowel pronunciation that’s linked to a speaker’s age, social class, gender, race and geography.
The research, presented June 29 at a meeting of the Acoustical Society of America, could help software developers create better speech recognition tools for smartphones and other devices. To understand the medley of southern vowel sounds, linguist Margaret Renwick of the University of Georgia in Athens dove into the Digital Archive of Southern Speech. The archive comprises almost 400 hours of interviews with 64 native Southerners representing a mix of ethnicities, social classes, education levels and ages.
Renwick’s analysis of more than 300,000 vowel sounds finds, for example, that Southern upper middle class women are often at the extreme end of variation in pronunciation. While Southern men and women are equally likely to shift the vowel in bet to “bay-ut,” upper middle class Southern women are more likely to stretch the vowel sound in bit to “bee-ut.” They are also most likely to pronounce bait as bite. The finding that women are more inclined to draw a sound out into two syllables — or change it entirely — is in line with other research suggesting that women are linguistic innovators, and less likely to adhere to the norms of standard American English, Renwick said.
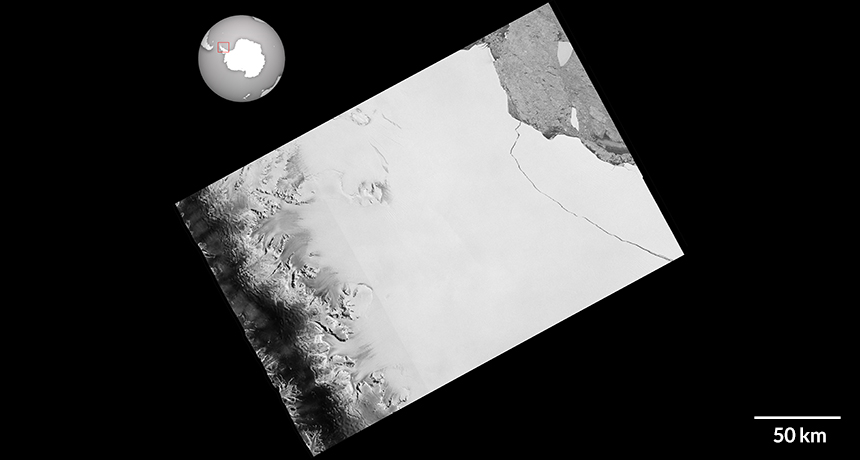
With a final rip, an iceberg roughly the size of Delaware has broken off Antarctica’s Larsen C ice shelf. Anticipated for weeks, the fracture is one of the largest calving events ever recorded.
On July 12, satellite images confirmed a nearly 5,800-square-kilometer, 1-trillion-metric-ton chunk of ice, equivalent to 12 percent of Larsen C’s total area, split from the ice shelf. “[We] have been surprised how long it took for the rift to break through the final few kilometers of ice,” Adrian Luckman, a glaciologist at Swansea University in Wales, said in a blogpost for Project MIDAS, which has been tracking the effects of a warming climate on the ice shelf. Now the focus will shift to the stability of the remaining ice shelf and the fate of the giant iceberg. Scientists had been monitoring Larsen C since 2014, when they noticed that a crack in the ice shelf had grown roughly 20 kilometers in less than nine months (SN: 7/25/15, p. 8). After a relative lull in 2015, the crack grew another 40 kilometers in 2016 and then 10 more in the first half of January 2017, bringing its total length to 175 kilometers. At that point, its tip was 20 kilometers from the Weddell Sea. The crack grew another 17 kilometers between May 25 and May 31 — at times traveling parallel to the edge and ultimately putting it within 13 kilometers of the ice front. Then, in late June, the outer part of the ice shelf picked up speed, putting new pressure on the crack and the entire shelf. “It won’t be long now,” Project Midas tweeted June 30. Added Luckman, also in a tweet: “The remaining ice is strained near to breaking point.”
Yet the vigil lasted nearly two more weeks. By July 6, the crack had come within 5 kilometers of the edge of the ice. Then, sometime between July 10 and July 12, it finally reached the water, allowing the huge hunk of ice to splinter off into the sea. The ice loss dramatically alters the landscape of Larsen C, Luckman notes. “Maps will need to be redrawn.” And that could be the least of the trouble ahead, says Adam Booth, a geophysicist at the University of Leeds in England also with Project MIDAS. “The calving event is significant because it is likely a precursor to something much bigger, potentially the collapse of the whole Larsen C ice shelf,” Booth says. The same thing happened to the neighboring Larsen B ice shelf in 2002, after it calved a Rhode Island-sized iceberg (SN: 3/30/02, p. 197).
“Glaciologists are keen to see how Larsen C will react,” says Luckman.
A complete collapse of Larsen C could have implications for sea level rise. Antarctica’s ice shelves act as buttresses, helping to slow the flow of the continent’s ice into the ocean. Since these shelves float on the water, calving icebergs don’t directly raise sea level. But calving or the collapse of an ice shelf allows glaciers and ice streams further inland to flow into the ocean, which can contribute to sea level rise.
Calving of icebergs is common, and over several decades, the shelves usually recover to their original size. But in the last two decades, ice shelves have instead continued to lose ice until collapsing, probably as a result of rising temperatures due to climate change, researchers suspect. In 2014, researchers concluded the collapse of Larsen B was the result of warming (SN: 10/18/14, p. 9).
Some computer simulations suggest Larsen C could suffer the same fate, possibly within a few years to decades, Luckman says. Still, the calving event that feeds a potential collapse may be hard to pin on climate change. “Not all ice-related stories have a clear global warming origin,” Luckman notes. Larsen C’s calving, he says, “may simply be a natural event that would have happened regardless of human activity.” Not everyone is convinced that Larsen C will fall apart completely. Researchers from Europe predict major changes to the shelf would happen only if it loses 55 percent of its ice. At that point, a significant amount of ice could ooze from glaciers into the ocean. Still, understanding what allowed the recent rift to grow and calve will “give us insight regarding other fractures or rifts on the shelf,” says geoscientist Dan McGrath of Colorado State University in Fort Collins. While McGrath says a collapse is “very unlikely,” he adds that “these other dormant rifts are in locations where if they reinitiated, the subsequent calving event would be worrisome for the shelf’s stability.”
Discrepancies in the predictions of Larsen C’s fate raise an important point, says Richard Alley, a geologist at Penn State. Researchers don’t understand ice shelf calving and collapsing enough predict how any one individual ice shelf will behave after a break.
“The Larsen C ice shelf is, of course, just one small part of Antarctica,” Booth says. “What is worrying is that we’re seeing trends in several ice shelves that tend towards decreasing stability. Should they continue along these trends, we could be seeing the start of increased mass loss from the Antarctic continent.”
A genetic-engineering tool designed to spread through a population like wildfire — eradicating disease and even whole invasive species — might be more easily thwarted than thought.
Resistance to the tools, called CRISPR gene drives, arose at high rates in experiments with Drosophila melanogaster fruit flies, researchers at Cornell University report July 20 in PLOS Genetics. Rates of resistance varied among strains of fruit flies collected around the world, from a low of about 4 percent in embryos from an Ithaca, N.Y., strain to a high of about 56 percent in Tasmanian fruit fly embryos. “At these rates, the constructs would not start spreading in the population,” says coauthor Philipp Messer, a population geneticist. “It might require quite a bit more work to get a gene drive that works at all.”
Gene drives are basically genetic copy-and-paste machines. These self-perpetuating machines are inherited by more than 50 percent of offspring of an individual carrying a gene drive. Working perfectly, they could transmit to 100 percent of offspring.
In its simplest form, a CRISPR gene drive consists of a piece of DNA that encodes both an enzyme called Cas9, which acts as molecular scissors, and a guide RNA that tells the Cas9 enzyme where to cut. That cutting may disrupt important genes. Researchers are experimenting with this as a way to sterilize malaria-carrying mosquitoes (SN Online: 12/7/15).
Some gene drives also carry a genetic payload. For instance, another approach to fighting malaria is to develop drives that carry genes to “vaccinate” mosquitoes against the disease (SN: 12/26/15, p. 6). Other drives might carry genes that make fluorescent proteins to indicate the gene drive’s presence; Messer and colleagues used such markers to follow two gene drives in fruit flies bred in the lab. When an organism carrying the tool mates with one that doesn’t, gene drives go to work. Inside the fertilized egg, guide RNAs shepherd Cas9 produced by the engineered mate to a spot where it cuts the other mate’s chromosome.
If everything works correctly, cells repair that break by copying the gene drive onto the cut chromosome. But the slice can also be fixed by gluing the cut ends back together. That regluing sometimes leads to mistakes that destroy Cas9’s cutting site, creating a chromosome that is resistant to the gene drive’s insertion.
In the fruit fly experiments, some mistakes created resistance during or before fertilization. Others took place in early embryos because cells produced Cas9 for too long, allowing the enzyme to chop chromosomes again and again, Messer and colleagues discovered. That was especially a problem when females produced Cas9, they found.
Some uses of gene drives, such as those that would sterilize or kill mosquitoes, can’t tolerate any amount of resistance no matter when it arises, Messer says. Because those types of gene drives damage the organism’s fertility or viability, mosquitoes carrying resistance would have an advantage and quickly outcompete insects vulnerable to the drives.
In a separate study posted June 14 at BioRxiv.org, Messer and colleagues tested several approaches to overcoming gene drive resistance. They found that using multiple guide RNAs and turning on Cas9 only in males could reduce resistance rates.
“This is a very important and elegant set of experiments,” says MIT evolutionary engineer Kevin Esvelt.
But the conclusions aren’t news to most gene drive researchers.
“We’re aware of all these problems, and the essence of how to deal with them hasn’t been changed by these studies,” says geneticist Ethan Bier of the University of California, San Diego. Bier and lab colleague Valentino Gantz created the first gene drive in fruit flies in 2015, and have worked with other researchers to develop gene drives that would prevent mosquitoes from carrying malaria (SN: 12/12/15, p. 16).
Messer’s group is, however, the first to experimentally confirm predictions about resistance and how to avoid it, Esvelt says. “They show what’s been apparent to some people in the field for a very long time.”
Some people might think that high rates of resistance mean that gene drives are safe to release because they won’t spread easily in the wild. But that notion is misguided, says Bier. Even if a gene drive is able to affect only a small percentage of a local pest population, it could still spread around the world, Esvelt adds. “It could still screw us all over in the current form.”
Researchers should continue to conduct gene drive experiments under tight containment, he and Bier caution.
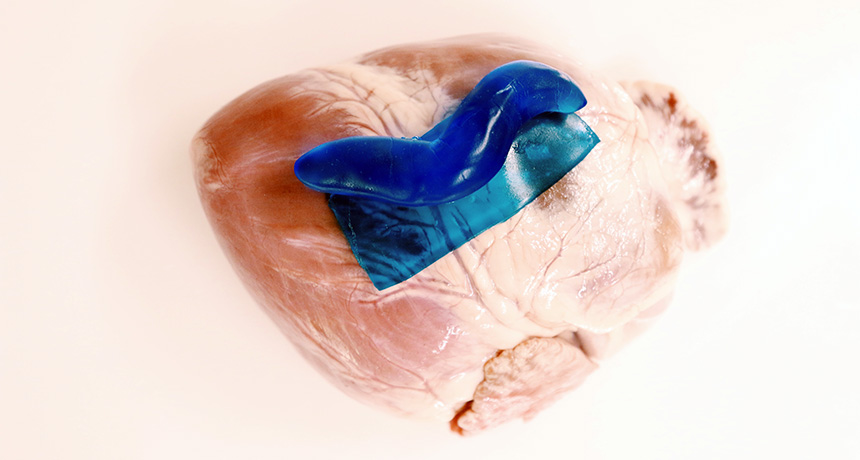
For a glue that holds up inside the body, turn to the humble slug, Arion subfuscus. A new super-sticky material mimics slug slime’s ability to stick on slick wet surfaces and could lead to more effective medical adhesives.
The material has two parts: a sticky layer that attaches to a surface, and a shock-absorbing layer that reduces strain. That makes the adhesive less likely to snap off.
Researchers tested the material as a surgical adhesive in a number of different scenarios: It stuck to pig skin and liver. It latched on to a beating pig’s heart, even when the surface was coated in blood. It sealed up a heart defect, preventing liquid from leaking even when the organ was inflated and deflated tens of thousands of times. And it was less toxic in the body than a commonly used commercialized tissue adhesive, researchers report July 28 in Science.
The researchers hope the material could someday be used in surgical procedures in place of invasive sutures and staples.
The company mice keep can change their behavior. In some ways, genetically normal littermates behave like mice that carry an autism-related mutation, despite not having the mutation themselves, scientists report.
The results, published July 31 in eNeuro, suggest that the social environment influences behavior in complex and important ways, says neuroscientist Alice Luo Clayton of the Simons Foundation Autism Research Initiative in New York City. The finding comes from looking past the mutated mice to their nonmutated littermates, which are usually not a subject of scrutiny. “People almost never look at it from that direction,” says Clayton, who wasn’t involved in the study. Researchers initially planned to investigate the social behavior of mice that carried a mutation found in some people with autism. Studying nonmutated mice wasn’t part of the plan. “We stumbled into this,” says study coauthor Stéphane Baudouin, a neurobiologist at Cardiff University in Wales.
Baudouin and colleagues studied groups of mice that had been genetically modified to lack neuroligin-3, a gene that is mutated in some people with autism. Without the gene, the mice didn’t have Neuroligin-3 in their brains, a protein that helps nerve cells communicate. Along with other behavioral quirks, these mice didn’t show interest in sniffing other mice, as expected. But Baudouin noticed that the behavior of the nonmutated control mice who lived with the neuroligin-3 mutants also seemed off. He suspected that the behavior of the mutated mice might be to blame.
Experiments confirmed this hunch. Usually, mice form strong social hierarchies, with the most aggressive and vocal males at the top. But in mixed groups of mutated and genetically normal male mice, there was no social hierarchy. “It’s flat,” Baudouin says.
Raised and housed together, the mutated and nonmutated mice all had less testosterone than nonmutated mice raised in genetically similar groups. The testosterone levels in both types of mice were comparable to those found in females — “one of the strongest and most surprising results,” Baudouin says.
The mice’s social curiosity was lacking, too. Usually, mice are interested in the smells of others, and will spend lots of time sniffing a cotton swab that had been swiped across the bedding of unfamiliar mice. But when given a choice of strange mouse scent or banana scent, the nonmutated littermates spent just as much time sniffing banana as did the mutant mice. When Baudouin and colleagues added back the missing Neuroligin-3 protein to parts of the mutant mice’s brains, aspects of their behavior normalized. The mice became interested in the odor from another mouse’s bedding, for instance. These behaviors also shifted in the mice’s nonmutated littermates. That experiment suggests that the missing protein — and the resulting abnormal behavior of the mutants — was to blame for their littermates’ abnormal actions.
Still, it’s hard to tease apart the mice’s roles, says behavioral neuroscientist Mu Yang of Columbia University. “It is a shared environment, and there is no sure way to tell who is influencing whom, or whether both parties are being impacted.”
Female mice that completely lacked the neuroligin-3 gene also influenced the behaviors of littermates that carried one mutated version of the gene, other behavior tests revealed. More experiments are needed to determine whether the social environment affects male and female mice differently, and if so, whether those differences relate to autism, says Luo Clayton.